

Clinical review: tuberculosis on the intensive care unit
- PMID: 24093433
- PMCID: PMC4056111
- DOI: 10.1186/cc12760
Clinical review: tuberculosis on the intensive care unit
Abstract
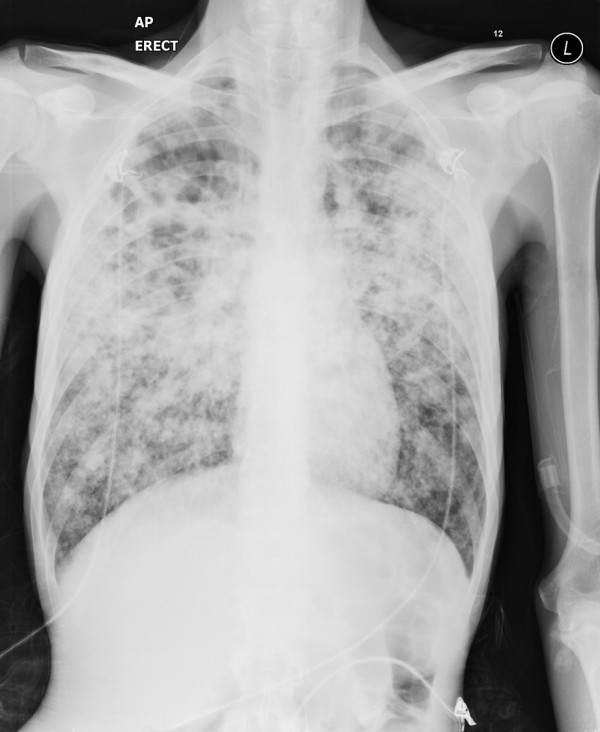
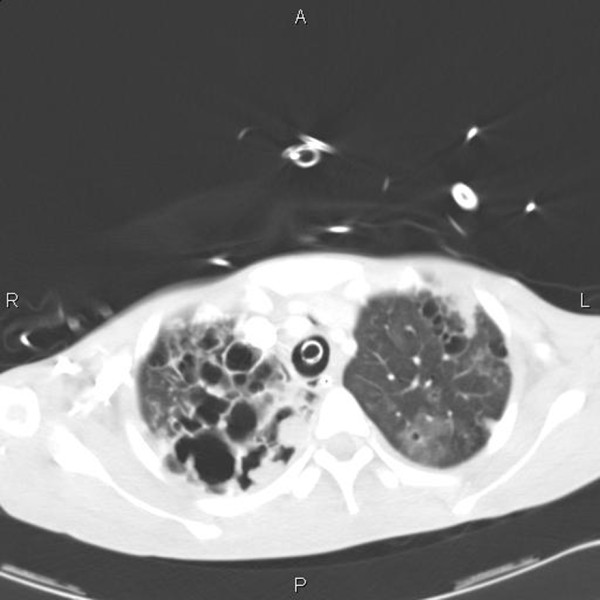
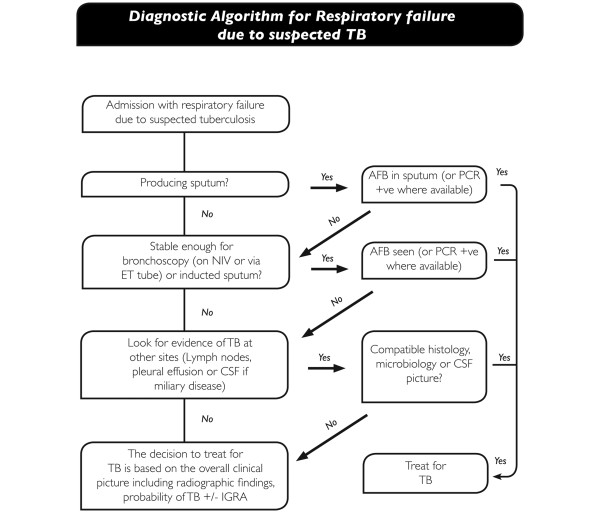
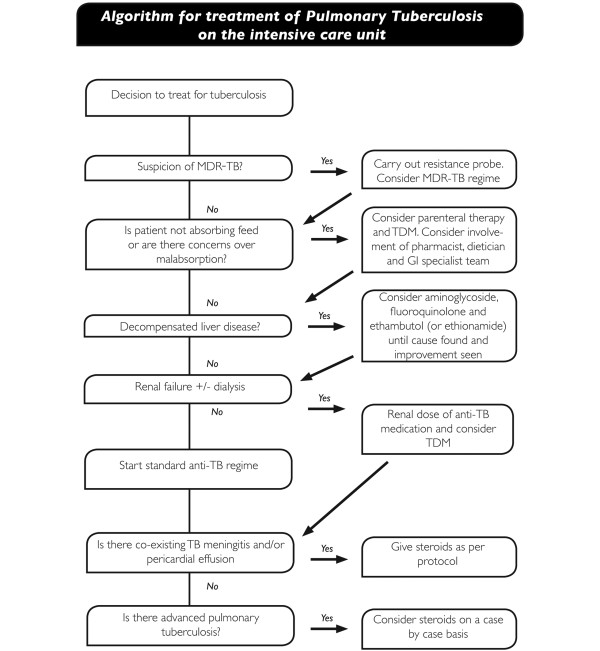
Rates of tuberculosis (TB) are increasing in most west European nations. Patients with TB can be admitted to an ICU for a variety of reasons, including respiratory failure, multiorgan failure and decreased consciousness associated with central nervous system disease. TB is a treatable disease but the mortality for patients admitted with TB to an ICU remains high. Management challenges exist in establishing a prompt diagnosis and administering effective treatment on the ICU with potentially poor gastric absorption and high rates of organ dysfunction and drug toxicity. In this review reasons for ICU admission, methods of achieving a confident diagnosis through direct and inferred methods, anti-tuberculosis treatment (including steroid and other adjuvant therapies) and specific management problems with particular relevance to the intensivist are discussed. The role of therapeutic drug monitoring, judicious use of alternative regimes in the context of toxicity or organ dysfunction and when to suspect paradoxical tuberculosis reactions are also covered. Diagnostic and therapeutic algorithms are proposed to guide ICU doctors in the management of this sometimes complicated disease.
Figures
References
-
- WHO. Global tuberculosis report 2012. http://www.who.int/tb/publications/global_report/en
-
- Pedrazzoli D, Fulton N, Anderson L, Lalor M, Abubakar A, Zenna D. Tuberculosis in the UK: 2012 report. http://www.hpa.org.uk/Publications/InfectiousDiseases/Tuberculosis/1206T...
-
- Lin SM, Wang TY, Liu WT. Predictive factors for mortality among non-HIV-infected patients with pulmonary tuberculosis and respiratory failure. Int J Tuberc Lung Dis. 2009;17:335–340. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
