

A combined anatomic and electrophysiologic substrate based approach for sudden cardiac death risk stratification
- PMID: 24093856
- PMCID: PMC4188429
- DOI: 10.1016/j.ahj.2013.06.023
A combined anatomic and electrophysiologic substrate based approach for sudden cardiac death risk stratification
Abstract
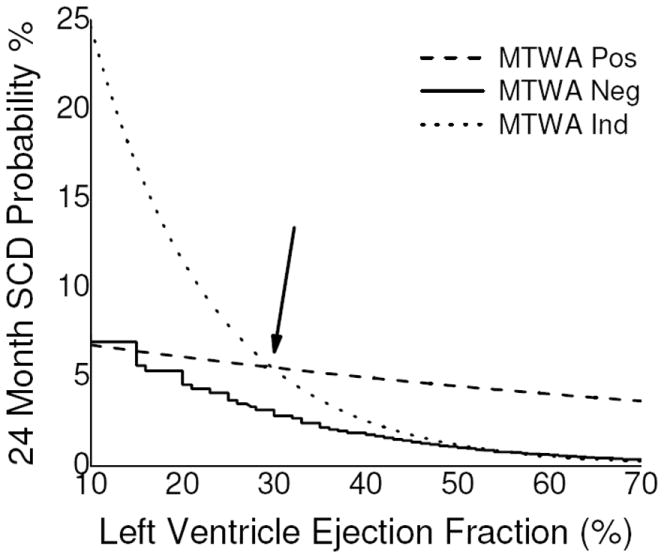
Background: Although left ventricular ejection fraction (LVEF) is the primary determinant for sudden cardiac death (SCD) risk stratification, in isolation, LVEF is a sub-optimal risk stratifier. We assessed whether a multi-marker strategy would provide more robust SCD risk stratification than LVEF alone.
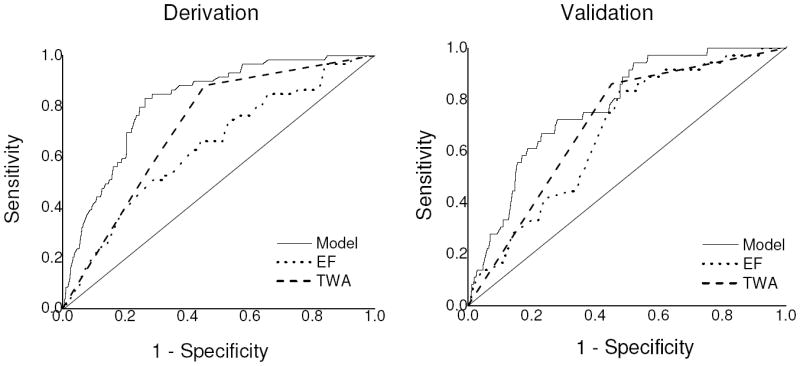
Methods: We collected patient-level data (n = 3355) from 6 studies assessing the prognostic utility of microvolt T-wave alternans (MTWA) testing. Two thirds of the group was used for derivation (n = 2242) and one-third for validation (n = 1113). The discriminative capacity of the multivariable model was assessed using the area under the receiver-operating characteristic curve (c-index). The primary endpoint was SCD at 24 months.
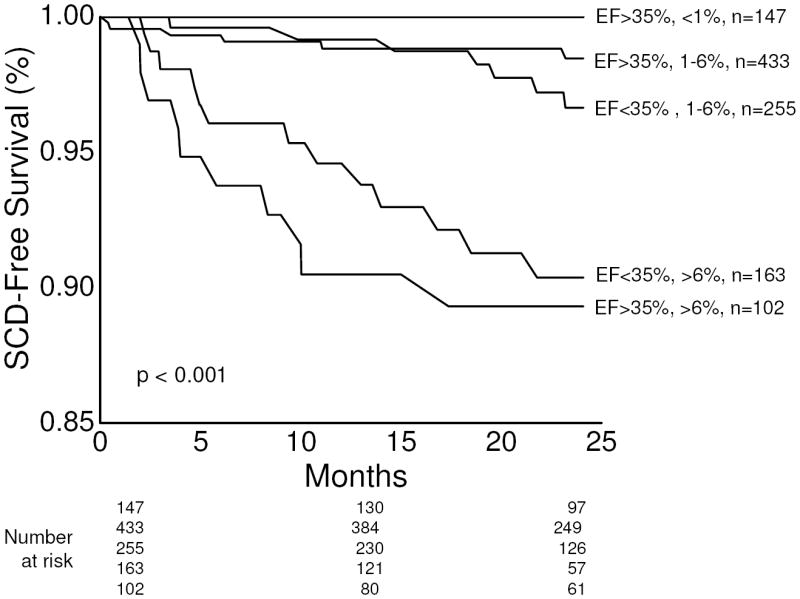
Results: In the derivation cohort, 59 patients experienced SCD by 24 months. Stepwise selection suggested that a model based on 3 parameters (LVEF, coronary artery disease and MTWA status) provided optimal SCD risk prediction. In the derivation cohort, the c-index of the model was 0.817, which was significantly better than LVEF used as a single variable (0.637, P < .001). In the validation cohort, 36 patients experienced SCD by 24 months. The c-index of the model for predicting the primary endpoint was again significantly better than LVEF alone (0.774 vs 0.671, P = .020).
Conclusions: A multivariable model based on presence of coronary artery disease, LVEF and MTWA status provides significantly more robust SCD risk prediction than LVEF as a single risk marker. These findings suggest that multi-marker strategies based on different aspects of the electro-anatomic substrate may be capable of improving primary prevention implantable cardioverter-defibrillator treatment algorithms.
© 2013 Mosby, Inc. All rights reserved.
Figures
References
-
- Moss AJ, Zareba W, Hall WJ, Klein H, Wilber DJ, Cannom DS, et al. Prophylactic implantation of a defibrillator in patients with myocardial infarction and reduced ejection fraction. The New England journal of medicine. 2002;346(12):877–83. - PubMed
-
- Bardy GH, Lee KL, Mark DB, Poole JE, Packer DL, Boineau R, et al. Amiodarone or an implantable cardioverter-defibrillator for congestive heart failure. The New England journal of medicine. 2005;352(3):225–37. - PubMed
-
- Epstein AE, DiMarco JP, Ellenbogen KA, Estes NA, 3rd, Freedman RA, Gettes LS, et al. ACC/AHA/HRS 2008 Guidelines for Device-Based Therapy of Cardiac Rhythm Abnormalities: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the ACC/AHA/NASPE 2002 Guideline Update for Implantation of Cardiac Pacemakers and Antiarrhythmia Devices): developed in collaboration with the American Association for Thoracic Surgery and Society of Thoracic Surgeons. Circulation. 2008;117(21):e350–408. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
