

Delays in appropriate antibiotic therapy for gram-negative bloodstream infections: a multicenter, community hospital study
- PMID: 24098449
- PMCID: PMC3789716
- DOI: 10.1371/journal.pone.0076225
Delays in appropriate antibiotic therapy for gram-negative bloodstream infections: a multicenter, community hospital study
Abstract
Background: Gram-negative bacterial bloodstream infection (BSI) is a serious condition with estimated 30% mortality. Clinical outcomes for patients with severe infections improve when antibiotics are appropriately chosen and given early. The objective of this study was to estimate the association of prior healthcare exposure on time to appropriate antibiotic therapy in patients with gram-negative BSI.
Method: We performed a multicenter cohort study of adult, hospitalized patients with gram-negative BSI using time to event analysis in nine community hospitals from 2003-2006. Event time was defined as the first administration of an antibiotic with in vitro activity against the infecting organism. Healthcare exposure status was categorized as community-acquired, healthcare-associated, or hospital-acquired. Time to appropriate therapy among groups of patients with differing healthcare exposure status was assessed using Kaplan-Meier analyses and multivariate Cox proportional hazards models.
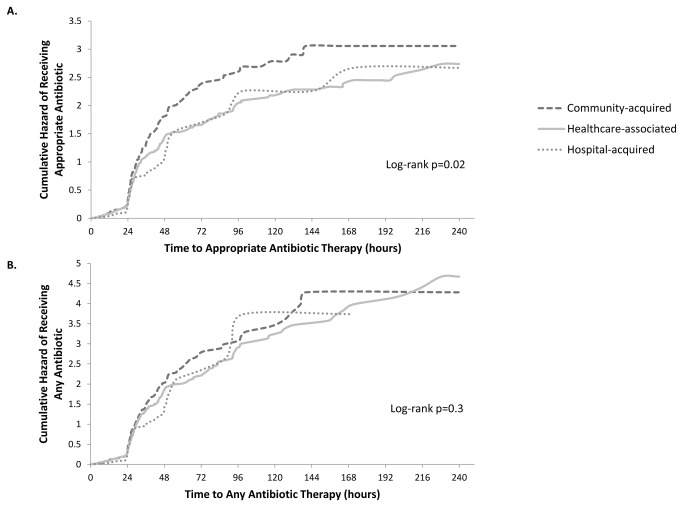
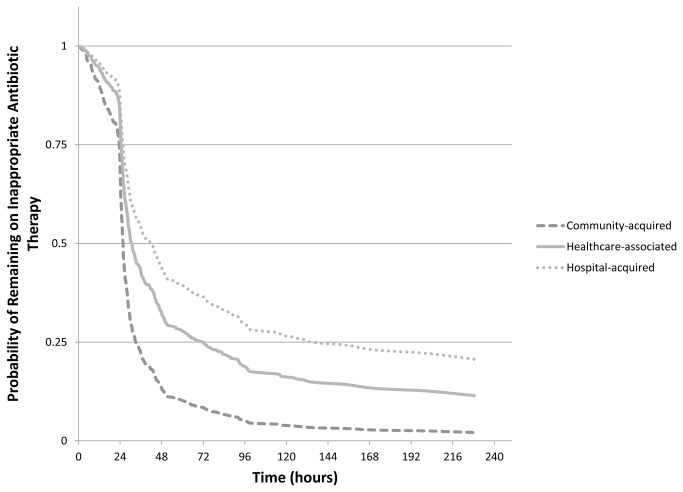
Results: The cohort included 578 patients with gram-negative BSI, including 320 (55%) healthcare-associated, 217 (38%) community-acquired, and 41 (7%) hospital-acquired infections. 529 (92%) patients received an appropriate antibiotic during their hospitalization. Time to appropriate therapy was significantly different among the groups of healthcare exposure status (log-rank p=0.02). Time to first antibiotic administration regardless of drug appropriateness was not different between groups (p=0.3). The unadjusted hazard ratios (HR) (95% confidence interval) were 0.80 (0.65-0.98) for healthcare-associated and 0.72 (0.63-0.82) for hospital-acquired, relative to patients with community-acquired BSI. In multivariable analysis, interaction was found between the main effect and baseline Charlson comorbidity index. When Charlson index was 3, adjusted HRs were 0.66 (0.48-0.92) for healthcare-associated and 0.57 (0.44-0.75) for hospital-acquired, relative to patients with community-acquired infections.
Conclusions: Patients with healthcare-associated or hospital-acquired BSI experienced delays in receipt of appropriate antibiotics for gram-negative BSI compared to patients with community-acquired BSI. This difference was not due to delayed initiation of antibiotic therapy, but due to the inappropriate choice of antibiotic.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
