

Defining the vulnerable period for re-establishment of Clostridium difficile colonization after treatment of C. difficile infection with oral vancomycin or metronidazole
- PMID: 24098459
- PMCID: PMC3788714
- DOI: 10.1371/journal.pone.0076269
Defining the vulnerable period for re-establishment of Clostridium difficile colonization after treatment of C. difficile infection with oral vancomycin or metronidazole
Abstract
Background: Clostridium difficile is an anaerobic, spore-forming bacterium that is the most common cause of healthcare-associated diarrhea in developed countries. A significant proportion of patients receiving oral vancomycin or metronidazole for treatment of Clostridium difficile infection (CDI) develop recurrences. However, the period of vulnerability to re-establishment of colonization by C. difficile after therapy is not well defined.
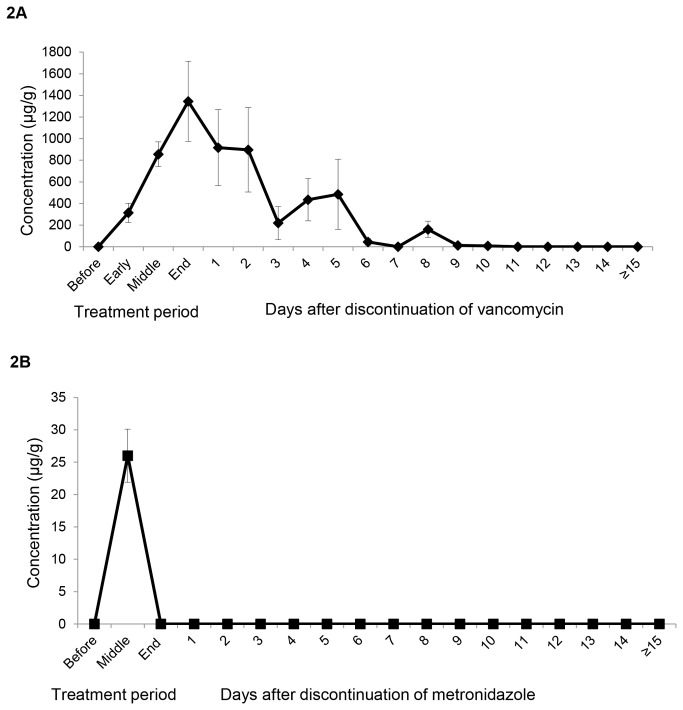
Principal findings: In a prospective study of CDI patients, we demonstrated that most vancomycin-treated patients maintained inhibitory concentrations of vancomycin in stool for 4 to 5 days after therapy, whereas metronidazole was only detectable during therapy. From the time of elimination of the antibiotics to 14 to 21 days after therapy, a majority of stool suspensions supported growth of C. difficile and deep 16S rRNA sequencing demonstrated persistent marked alteration of the indigenous microbiota. By 21 to 28 days after completion of CDI treatment, a majority of stool suspensions inhibited growth of C. difficile and there was evidence of some recovery of the microbiota.
Conclusions: These data demonstrate that there is a vulnerable period for re-establishment of C. difficile colonization after CDI treatment that begins within a few days after discontinuation of treatment and extends for about 3 weeks in most patients.
Conflict of interest statement
Figures





References
-
- Cohen SH, Gerding DN, Johnson S, Kelly CP, Loo VG et al. (2010) Clinical practice guidelines for Clostridium difficile infection in adults: 2010 update by the Society for Healthcare Epidemiology of America (SHEA) and the Infectious Diseases Society of America (IDSA). Infect Control Hosp Epidemiol 31: 431-455. doi:10.1086/651706. PubMed: 20307191. - DOI - PubMed
-
- Al-Nassir WN, Sethi AK, Li Y, Pultz MJ, Riggs MM et al. (2008) Both oral metronidazole and oral vancomycin promote persistent overgrowth of vancomycin-resistant enterococci during treatment of Clostridium difficile-associated disease. Antimicrob Agents Chemother 52: 2403-2406. doi:10.1128/AAC.00090-08. PubMed: 18443120. - DOI - PMC - PubMed
-
- Sethi AK, Al-Nassir WN, Nerandzic MM, Donskey CJ (2009) Skin and environmental contamination with vancomycin-resistant enterococci in patients receiving oral metronidazole or oral vancomycin treatment for Clostridium difficile-associated disease. Infect Control Hosp Epidemiol 30: 13-17. doi:10.1086/592710. PubMed: 19046063. - DOI - PubMed
-
- Edlund C, Barkholt L, Olsson-Liljequist B, Nord CE (1997) Effect of vancomycin on intestinal flora of patients who previously received antimicrobial therapy. Clin Infect Dis 25: 729-732. doi:10.1086/513755. PubMed: 9314469. - DOI - PubMed
-
- Louie TJ, Emery J, Krulicki W, Byrne B, Mah M (2009) OPT-80 eliminates Clostridium difficile and is sparing of Bacteroides species during treatment of C. difficile infection. Antimicrob Agents Chemother 53: 261-263. doi:10.1128/AAC.01443-07. PubMed: 18955523. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
