

Single incision versus conventional laparoscopic cholecystectomy outcomes: a meta-analysis of randomized controlled trials
- PMID: 24098522
- PMCID: PMC3788730
- DOI: 10.1371/journal.pone.0076530
Single incision versus conventional laparoscopic cholecystectomy outcomes: a meta-analysis of randomized controlled trials
Abstract
Background: Previous meta-analyses that compared the outcome of SILC and CLC have not presented consistent conclusions. This meta-analysis was performed after adding many recent RCTs, to clarify this issue.
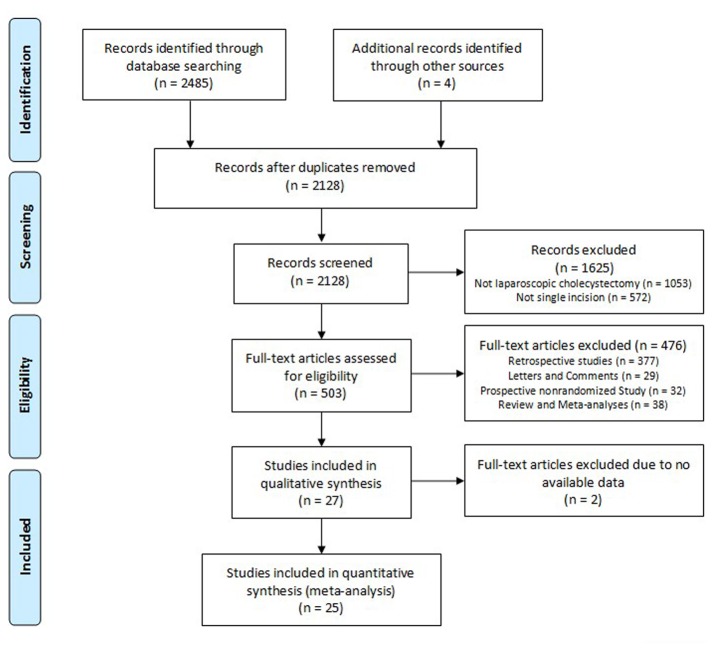
Methods: Relevant articles published in English were identified by searching PubMed, Embase, Web of Knowledge, and the Cochrane Controlled Trial Register from January 1997 to February 2013. Reference lists of the retrieved articles were reviewed to identify additional articles. Primary outcomes (postoperative pain scores, cosmetic score, and length of incision) and secondary outcomes (operating time, blood loss, conversion rates, postoperative complications, postoperative hospital stay, time to initial oral intake, and time to resume work) were pooled. Quantitative variables were calculated using the weighted mean difference (WMD), and qualitative variables were pooled using odds ratios (OR).
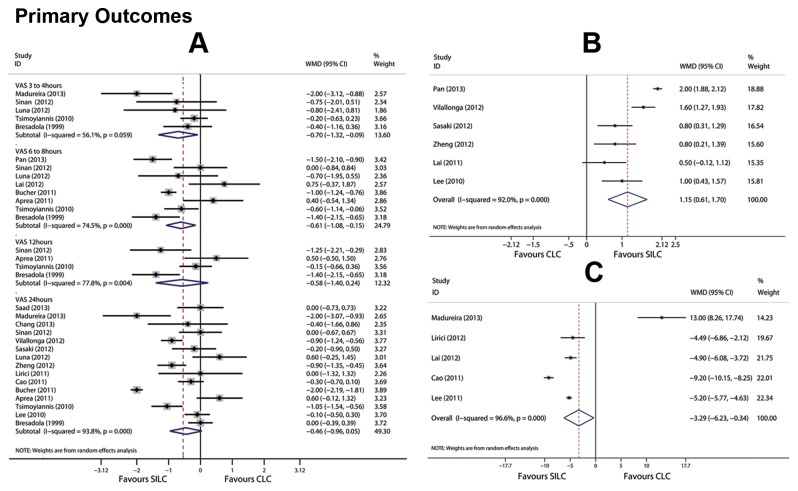
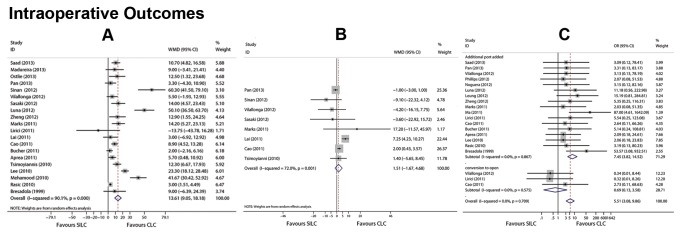
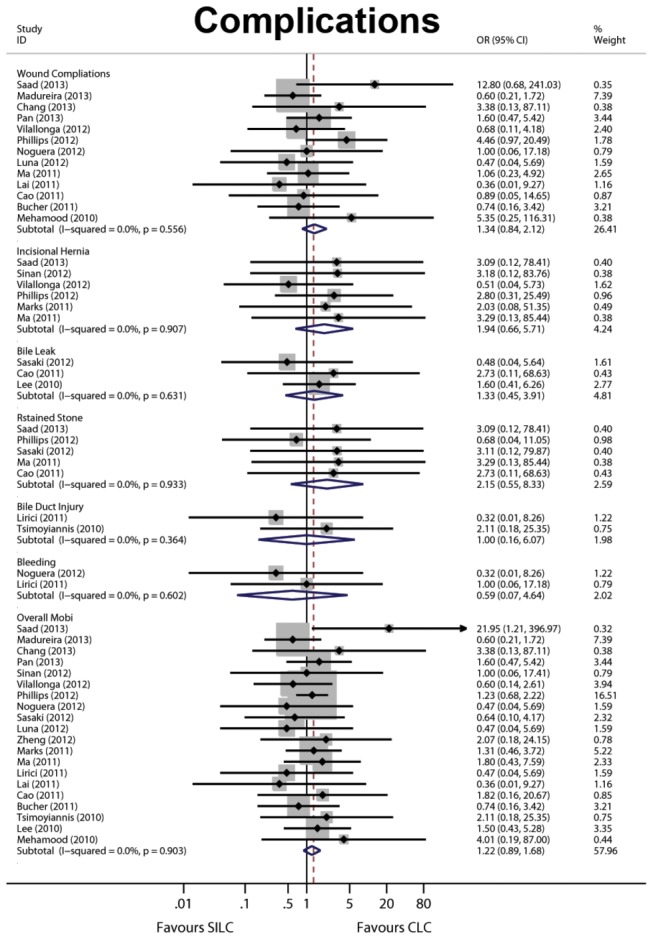
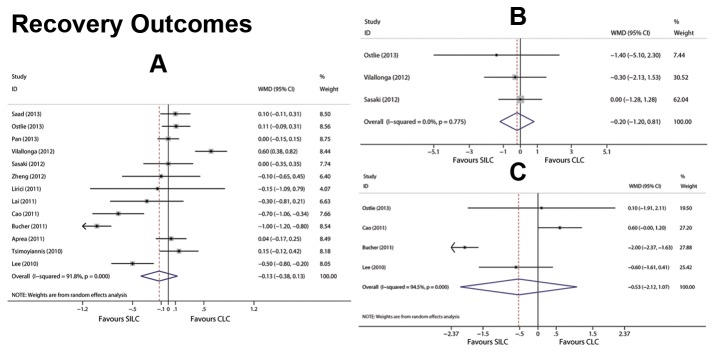
Results: 25 appropriate RCTs were identified from 2128 published articles. 1841 patients were treated, 944 with SILC and 897 with CLC. SILC was superior to CLC in cosmetic score (WMD = 1.155, P<0.001), shorter length of incision (WMD = -3.285, P = 0.029), and postoperative pain within 12 h (VAS in 3-4 h, WMD = -0.704, P = 0.026; VAS in 6-8 h, WMD = -0.613, P = 0.010). CLC was superior to SILC in operating time (OT) (WMD = 13.613, P<0.001) and need of additional instruments (OR = 7.448, P<0.001). Other secondary outcomes were similar.
Conclusions: SILC offered a better cosmetic result and less postoperative pain for patients with uncomplicated cholelithiasis or polypoid lesions of the gallbladder. However, SILC was associated with a longer OT and required additional instruments.
Conflict of interest statement
Figures
References
-
- Navarra G, Pozza E, Occhionorelli S, Carcoforo P, Donini I (1997) One-wound laparoscopic cholecystectomy. Br J Surg 84: 695. doi:10.1002/bjs.1800840536. PubMed: 9171771. - DOI - PubMed
-
- Joseph S, Moore BT, Sorensen GB, Earley JW, Tang F et al. (2011) Single-incision laparoscopic cholecystectomy: a comparison with the gold standard. Surg Endosc 25: 3008-3015. doi:10.1007/s00464-011-1661-x. PubMed: 21487878. - DOI - PubMed
-
- Hauters P, Auvray S, Cardin JL, Papillon M, Delaby J et al. (2013) Comparison between single-incision and conventional laparoscopic cholecystectomy: a prospective trial of the Club Coelio. Surg Endosc 27: 1689-1694. doi:10.1007/s00464-012-2657-x. PubMed: 23224032. - DOI - PubMed
-
- Solomon D, Shariff AH, Silasi DA, Duffy AJ, Bell RL et al. (2012) Transvaginal cholecystectomy versus single-incision laparoscopic cholecystectomy versus four-port laparoscopic cholecystectomy: a prospective cohort study. Surg Endosc 26: 2823-2827. doi:10.1007/s00464-012-2253-0. PubMed: 22549370. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
