

Changes in first-line cART regimens and short-term clinical outcome between 1996 and 2010 in The Netherlands
- PMID: 24098764
- PMCID: PMC3786897
- DOI: 10.1371/journal.pone.0076071
Changes in first-line cART regimens and short-term clinical outcome between 1996 and 2010 in The Netherlands
Abstract
Objectives: Document progress in HIV-treatment in The Netherlands since 1996 by reviewing changing patterns of cART use and relating those to trends in patients' short-term clinical outcomes between 1996 and 2010.
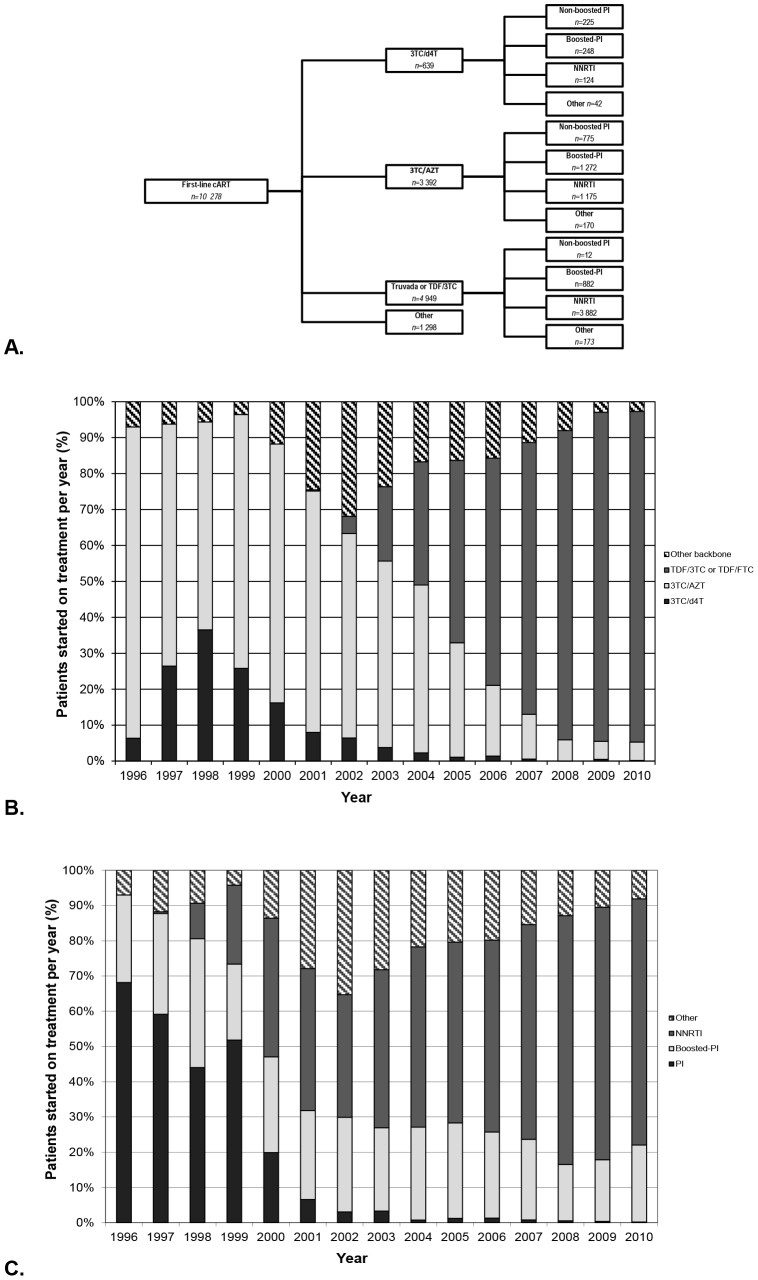
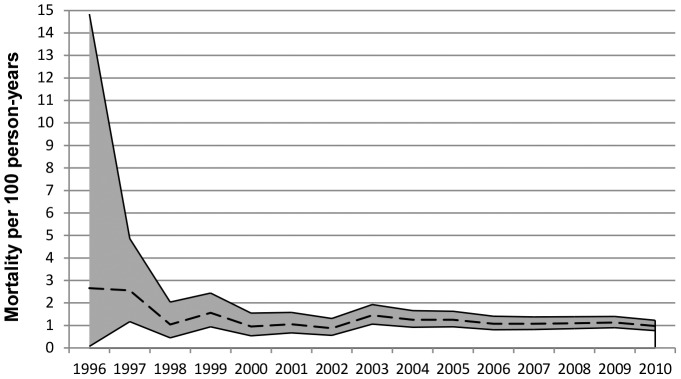
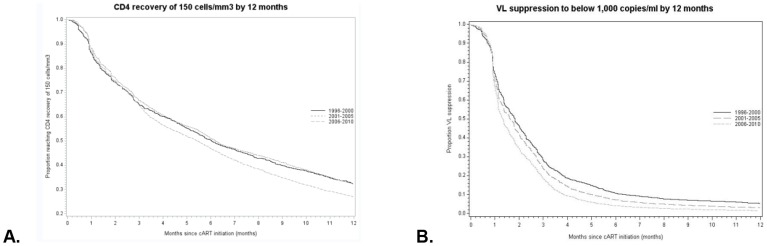
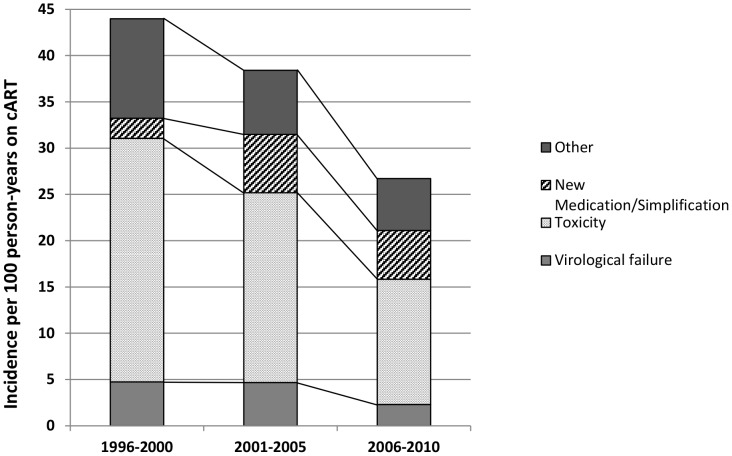
Design and methods: 1996-2010 data from 10,278 patients in the Dutch ATHENA national observational cohort were analysed. The annual number of patients starting a type of regimen was quantified. Trends in the following outcomes were described: i) recovery of 150 CD4 cells/mm(3) within 12 months of starting cART; ii) achieving viral load (VL) suppression ≤1,000 copies/ml within 12 months of starting cART; iii) switching from first-line to second-line regimen within three years of starting treatment; and iv) all-cause mortality rate per 100 person-years within three years of starting treatment.
Results: Between 1996 and 2010, first-line regimens changed from lamivudine/zidovudine-based or lamivudine/stavudine-based regimens with unboosted-PIs to tenofovir with either emtricitabine or lamivudine with NNRTIs. Mortality rates did not change significantly over time. VL suppression and CD4 recovery improved over time, and the incidence of switching due to virological failure and toxicity more than halved between 1996 and 2010. These effects appear to be related to the use of new regimens rather than improvements in clinical care.
Conclusion: The use of first-line cART in the Netherlands closely follows changes in guidelines, to the benefit of patients. While there was no significant improvement in mortality, newer drugs with better tolerability and simpler dosing resulted in improved immunological and virological recovery and reduced incidences of switching due to toxicity and virological failure.
Conflict of interest statement
Figures
References
-
- FDA (2012) Antiretroviral drugs used in the treatment of HIV infection - Drugs Used in the Treatment of HIV Infection. Available: http://www.fda.gov/forconsumers/byaudience/forpatientadvocates/hivandaid.... Accessed 12 June 2010.
-
- Robbins GK, De Gruttola V, Shafer RW, Smeaton LM, Snyder SW, et al. (2003) Comparison of sequential three-drug regimens as initial therapy for HIV-1 infection. N Engl J Med 349: 2293–2303 doi:10.1056/NEJMoa030264 - DOI - PMC - PubMed
-
- Dubé M, Zackin R, Tebas R, Roubenoff R, Mulligan K, et al. (2002) Prospective Study of Regional Body Composition in Antiretroviral-Naive Subjects Randomized to Receive Zidovudine + Lamivudine or Didanosine + Stavudine Combined With Nelfinavir, Efavirenz or Both: A5005s, a Substudy of ACTG 384. Antiretroviral Therapy 7: L27.
-
- Gallant JE, Staszewski S, Pozniak AL, DeJesus E, Suleiman JMAH, et al. (2004) Efficacy and safety of tenofovir DF vs stavudine in combination therapy in antiretroviral-naive patients: a 3-year randomized trial. JAMA 292: 191–201 doi:10.1001/jama.292.2.191 - DOI - PubMed
-
- Gallant JE, DeJesus E, Arribas JR, Pozniak AL, Gazzard B, et al. (2006) Tenofovir DF, emtricitabine, and efavirenz vs. zidovudine, lamivudine, and efavirenz for HIV. N Engl J Med 354: 251–260 doi:10.1056/NEJMoa051871 - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
