

Review
doi: 10.1161/CIRCULATIONAHA.113.002114.
Coronary artery revascularization in patients with diabetes mellitus
Affiliations
- PMID: 24100481
- PMCID: PMC3901842
- DOI: 10.1161/CIRCULATIONAHA.113.002114
Item in Clipboard
Review
Coronary artery revascularization in patients with diabetes mellitus
Circulation.
.
No abstract available
Keywords: diabetes mellitus; myocardial revascularization; percutaneous coronary intervention.
Figures
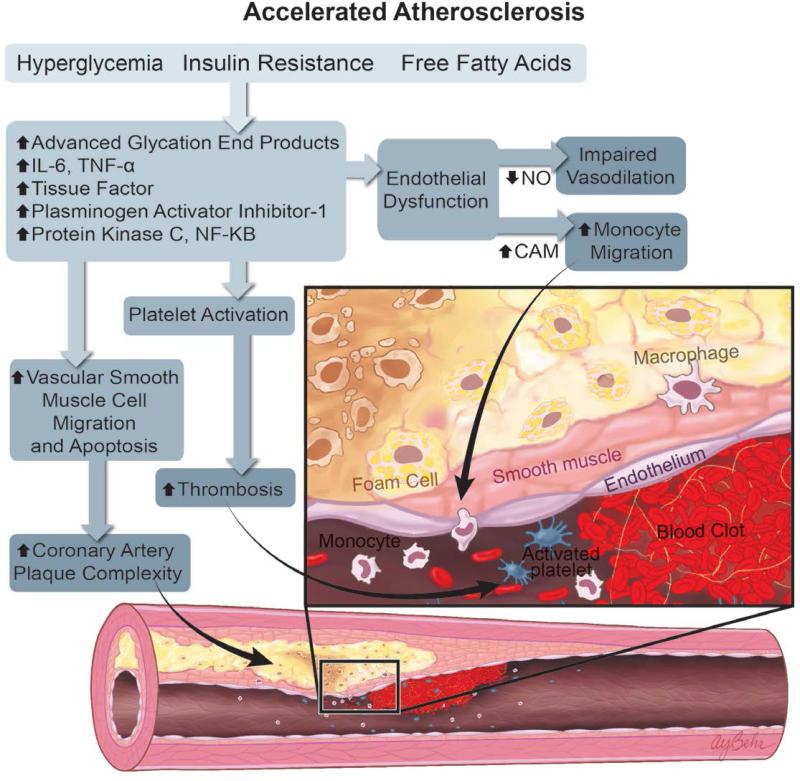
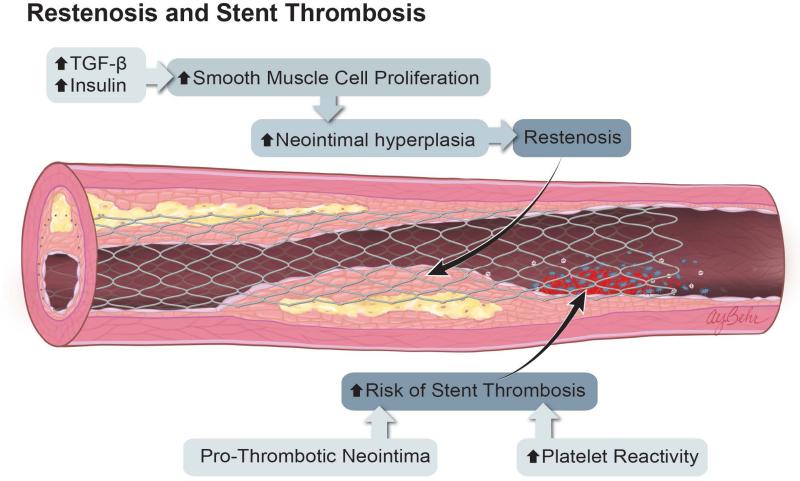
Mechanisms of Atherosclerosis and Restenosis in Diabetes. A. The combination of hyperglycemia, insulin resistance, and increased circulating free fatty acids activate multiple inflammatory pathways, leading to endothelial dysfunction, increased monocyte activation and localization to sites of nascent plaque, increased vascular smooth muscle cell migration, and apoptosis. These inflammatory pathways also increase platelet activation, leading to an increased risk of atherothrombosis and coronary artery plaque complexity. B. After percutaneous coronary intervention, elevated levels of insulin and TGF-β promote greater smooth muscle cell proliferation, neointimal hyperplasia, and restenosis. Patients with DM may also have prothrombotic neointima, as well as increased platelet reactivity. The sum of these effects results in an increased risk of stent thrombosis.
Mechanisms of Atherosclerosis and Restenosis in Diabetes. A. The combination of hyperglycemia, insulin resistance, and increased circulating free fatty acids activate multiple inflammatory pathways, leading to endothelial dysfunction, increased monocyte activation and localization to sites of nascent plaque, increased vascular smooth muscle cell migration, and apoptosis. These inflammatory pathways also increase platelet activation, leading to an increased risk of atherothrombosis and coronary artery plaque complexity. B. After percutaneous coronary intervention, elevated levels of insulin and TGF-β promote greater smooth muscle cell proliferation, neointimal hyperplasia, and restenosis. Patients with DM may also have prothrombotic neointima, as well as increased platelet reactivity. The sum of these effects results in an increased risk of stent thrombosis.
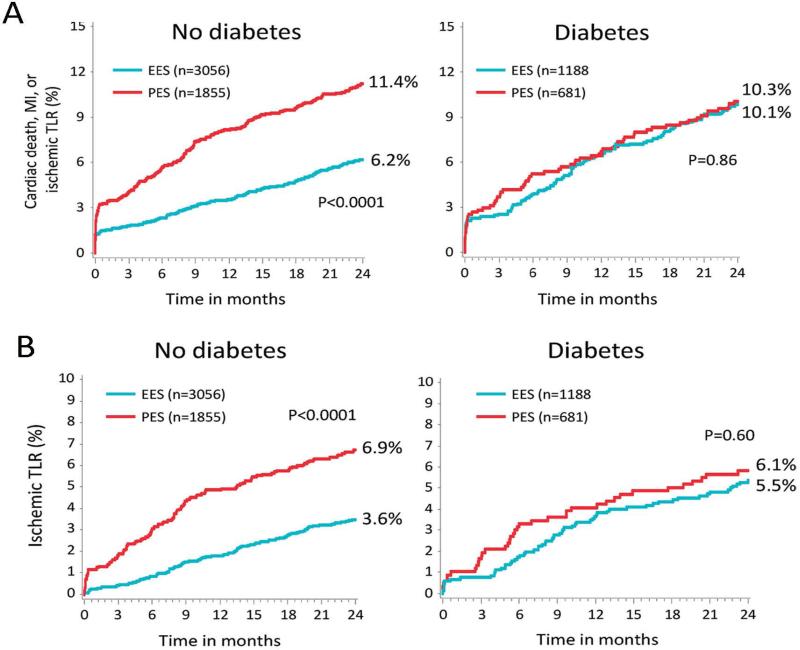
Differential Outcomes After PCI Among Patients with and without Diabetes in the SPIRIT and COMPARE Trials. Pooled analysis of the SPIRIT and COMPARE trials demonstrate a significant interaction effect of diabetes on the outcomes of everolimus-eluting stents (EES) vs. paclitaxel-eluting stents (PES). Top panel: Among patients without diabetes, the rates of cardiac death, MI, or ischemic TLR were significantly lower for EES compared to PES. In comparison, there was no difference in outcomes of EES vs. PES among patients with DM. Bottom panel: Among patients without diabetes, EES were associated with significantly decreased rates of ischemic TLR. There was no difference in rates of ischemic TLR among patients with diabetes. (Reproduced, with permission, from Stone et al, Circulation 2011;124:893-900.)
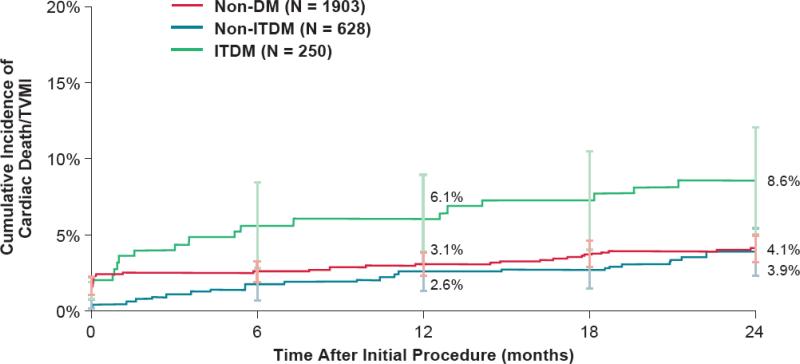
Outcomes After PCI Among Patients with Diabetes Treated with Resolute Zotarolimus-Eluting Stents. During two-year follow-up, the rates of cardiac death or target vessel MI were similar between patients without diabetes and those with diabetes who did not require treatment with insulin (non-ITDM). In comparison, patients with diabetes who required treatment with insulin (ITDM) had significantly higher rates of cardiac death or target vessel MI at two years of follow-up. (Reproduced, with permission, from Silber et al J. Am. Coll. Cardiol. Intv, 2013; 6:357-368.)
References
-
- Wild S, Roglic G, Green A, Sicree R, King H. Global prevalence of diabetes: Estimates for the year 2000 and projections for 2030. Diabetes Care. 2004;27:1047–1053. - PubMed
-
- Center for Disease Control and Prevention. Atlanta G. National diabetes fact sheet: National estimates and general information on diabetes and prediabetes in the us 2011. US Department of Health and Human Services; 2011.
-
- Hammoud T, Tanguay JF, Bourassa MG. Management of coronary artery disease: Therapeutic options in patients with diabetes. J Am Coll Cardiol. 2000;36:355–365. - PubMed
-
- Schramm TK, Gislason GH, Kober L, Rasmussen S, Rasmussen JN, Abildstrom SZ, Hansen ML, Folke F, Buch P, Madsen M, Vaag A, Torp-Pedersen C. Diabetes patients requiring glucose-lowering therapy and nondiabeticsf with a prior myocardial infarction carry the same cardiovascular risk: A population study of 3.3 million people. Circulation. 2008;117:1945–1954. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
