

Randomized trial of hypofractionated external-beam radiotherapy for prostate cancer
- PMID: 24101042
- PMCID: PMC3805927
- DOI: 10.1200/JCO.2013.51.1972
Randomized trial of hypofractionated external-beam radiotherapy for prostate cancer
Abstract
Purpose: To determine if escalated radiation dose using hypofractionation significantly reduces biochemical and/or clinical disease failure (BCDF) in men treated primarily for prostate cancer.
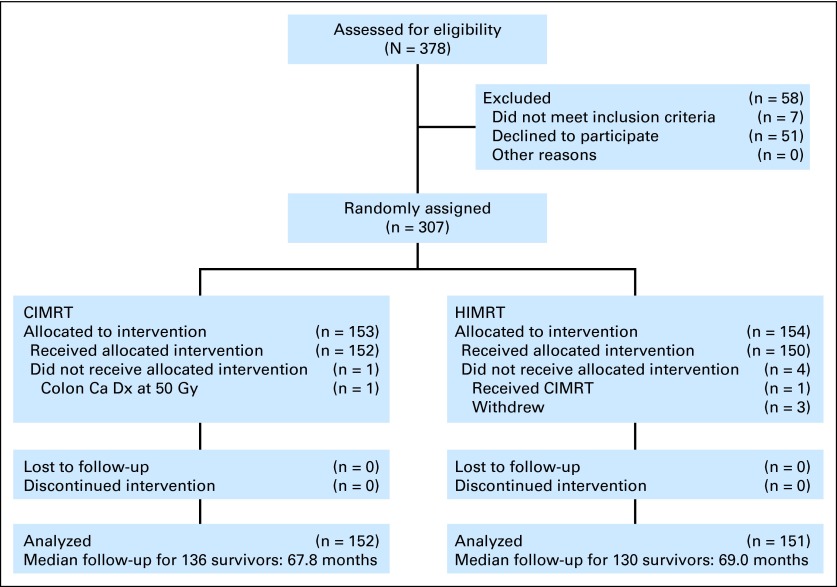
Patients and methods: Between June 2002 and May 2006, men with favorable- to high-risk prostate cancer were randomly allocated to receive 76 Gy in 38 fractions at 2.0 Gy per fraction (conventional fractionation intensity-modulated radiation therapy [CIMRT]) versus 70.2 Gy in 26 fractions at 2.7 Gy per fraction (hypofractionated IMRT [HIMRT]); the latter was estimated to be equivalent to 84.4 Gy in 2.0 Gy fractions. High-risk patients received long-term androgen deprivation therapy (ADT), and some intermediate-risk patients received short-term ADT. The primary end point was the cumulative incidence of BCDF. Secondarily, toxicity was assessed.
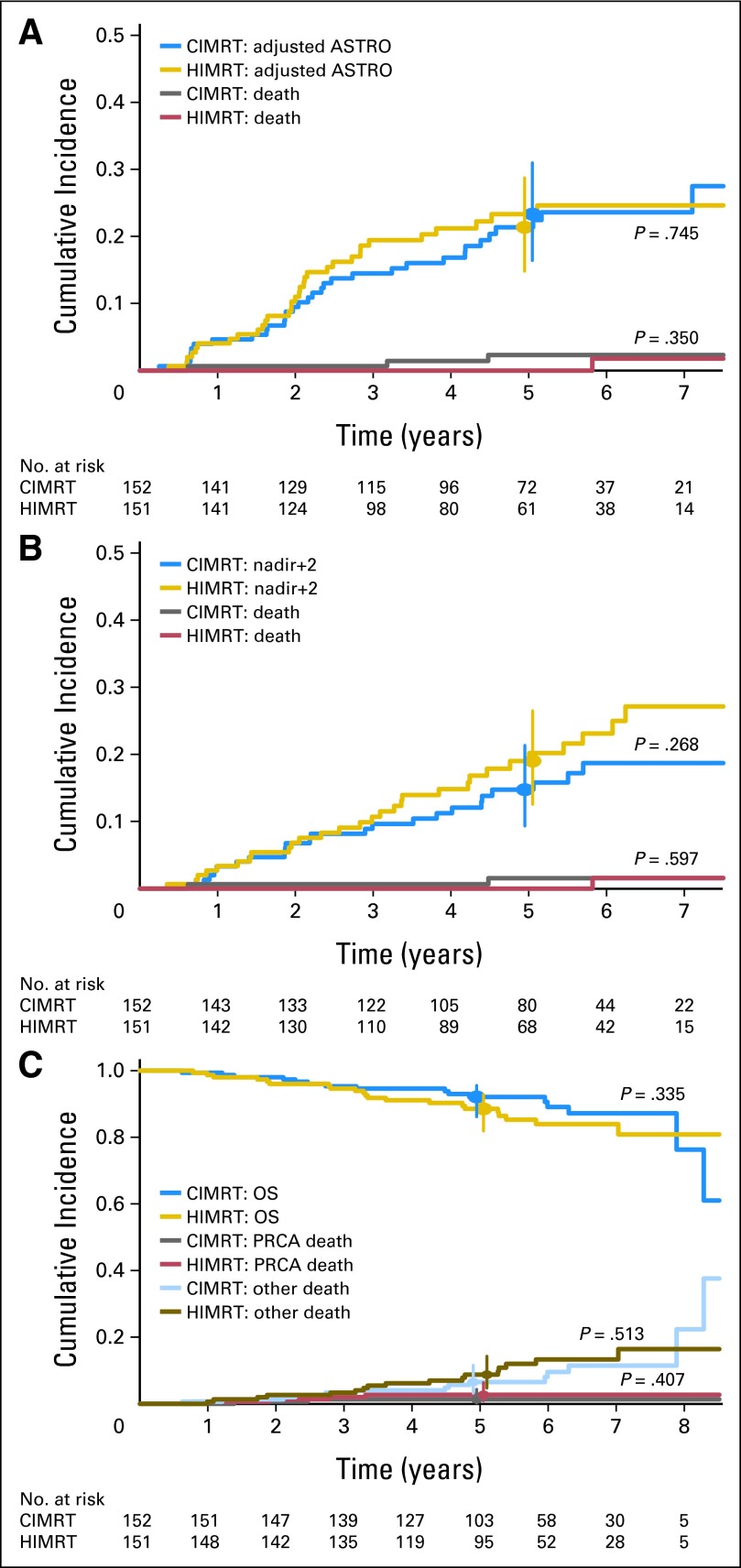
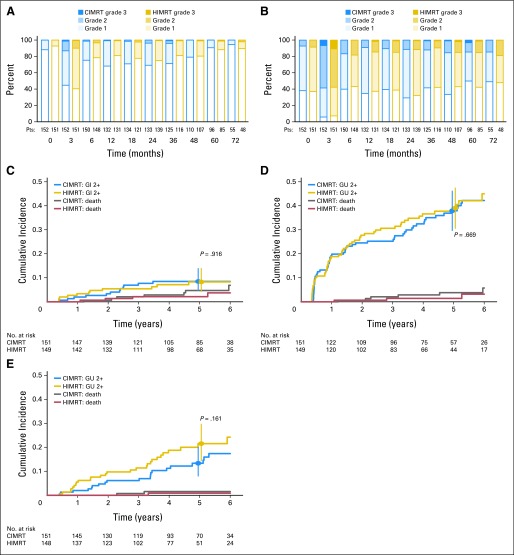
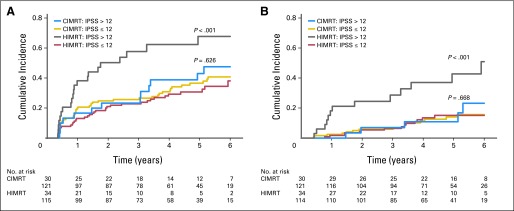
Results: There were 303 assessable patients with a median follow-up of 68.4 months. No significant differences were seen between the treatment arms in terms of the distribution of patients by clinicopathologic or treatment-related (ADT use and length) factors. The 5-year rates of BCDF were 21.4% (95% CI, 14.8% to 28.7%) for CIMRT and 23.3% (95% CI, 16.4% to 31.0%) for HIMRT (P = .745). There were no statistically significant differences in late toxicity between the arms; however, in subgroup analysis, patients with compromised urinary function before enrollment had significantly worse urinary function after HIMRT.
Conclusion: The hypofractionation regimen did not result in a significant reduction in BCDF; however, it is delivered in 2.5 fewer weeks. Men with compromised urinary function before treatment may not be ideal candidates for this approach.
Trial registration: ClinicalTrials.gov NCT00062309.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest and author contributions are found at the end of this article.
Figures
Comment in
-
Prostate cancer and the hypofractionation hypothesis.J Clin Oncol. 2013 Nov 1;31(31):3849-51. doi: 10.1200/JCO.2013.52.4942. Epub 2013 Oct 7. J Clin Oncol. 2013. PMID: 24101055 No abstract available.
-
Re: Randomized trial of hypofractionated external-beam radiotherapy for prostate cancer.J Urol. 2014 Apr;191(4):983-5. doi: 10.1016/j.juro.2014.01.074. Epub 2014 Jan 17. J Urol. 2014. PMID: 24703117 No abstract available.
-
Is there any benefit from hypofractionation in external-beam irradiation for prostate cancer?J Clin Oncol. 2014 Jun 10;32(17):1851-2. doi: 10.1200/JCO.2013.54.4247. Epub 2014 Apr 28. J Clin Oncol. 2014. PMID: 24778396 Free PMC article. No abstract available.
-
Hypofractionated radiation therapy for prostate cancer: more food for thought from recent trial.J Clin Oncol. 2014 Jun 10;32(17):1852-3. doi: 10.1200/JCO.2013.54.8123. Epub 2014 Apr 28. J Clin Oncol. 2014. PMID: 24778400 No abstract available.
-
Reply to M.J. Brenner et al and I.R. Vogelius et al.J Clin Oncol. 2014 Jun 10;32(17):1853-4. doi: 10.1200/JCO.2013.54.7729. Epub 2014 Apr 28. J Clin Oncol. 2014. PMID: 24778402 No abstract available.
References
-
- Kuban DA, Tucker SL, Dong L, et al. Long-term results of the M. D. Anderson randomized dose-escalation trial for prostate cancer. Int J Radiat Oncol Biol Phys. 2008;70:67–74. - PubMed
-
- Al-Mamgani A, van Putten WL, Heemsbergen WD, et al. Update of Dutch multicenter dose-escalation trial of radiotherapy for localized prostate cancer. Int J Radiat Oncol Biol Phys. 2008;72:980–988. - PubMed
-
- Khoo V, Pollack A, Cowen D, et al. Relationship of Ki-67 labeling index to DNA-ploidy, S-phase fraction, and outcome in prostate cancer treated with radiotherapy. Prostate. 1999;41:166–172. - PubMed
-
- Haustermans K, Hofland I, Poppel H, et al. Cell kinetic measurements in prostate cancer. Int J Radiat Oncol Biol Phys. 1997;37:1067–1070. - PubMed
-
- Duchesne GM, Peters LJ. What is the alpha/beta ratio for prostate cancer? Rationale for hypofractionated high-dose-rate brachytherapy. Int J Radiat Oncol Biol Phys. 1999;44:747–748. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
