

Defining high risk: cost-effectiveness of extended-duration thromboprophylaxis following major oncologic abdominal surgery
- PMID: 24101450
- PMCID: PMC4652588
- DOI: 10.1007/s11605-013-2373-4
Defining high risk: cost-effectiveness of extended-duration thromboprophylaxis following major oncologic abdominal surgery
Abstract
Purpose: Extended-duration thromboprophylaxis (EDTPPX) is the practice of prescribing antithrombotic therapy for 21 days after discharge, commonly used in surgical patients who are at high risk for venothromboembolism (VTE). While guidelines recommend EDTPPX, criteria are vague due to a paucity of data. The criteria can be further informed by cost-effectiveness thresholds. This study sought to determine the VTE incidence threshold for the cost-effectiveness of EDTPPX compared to inpatient prophylaxis.
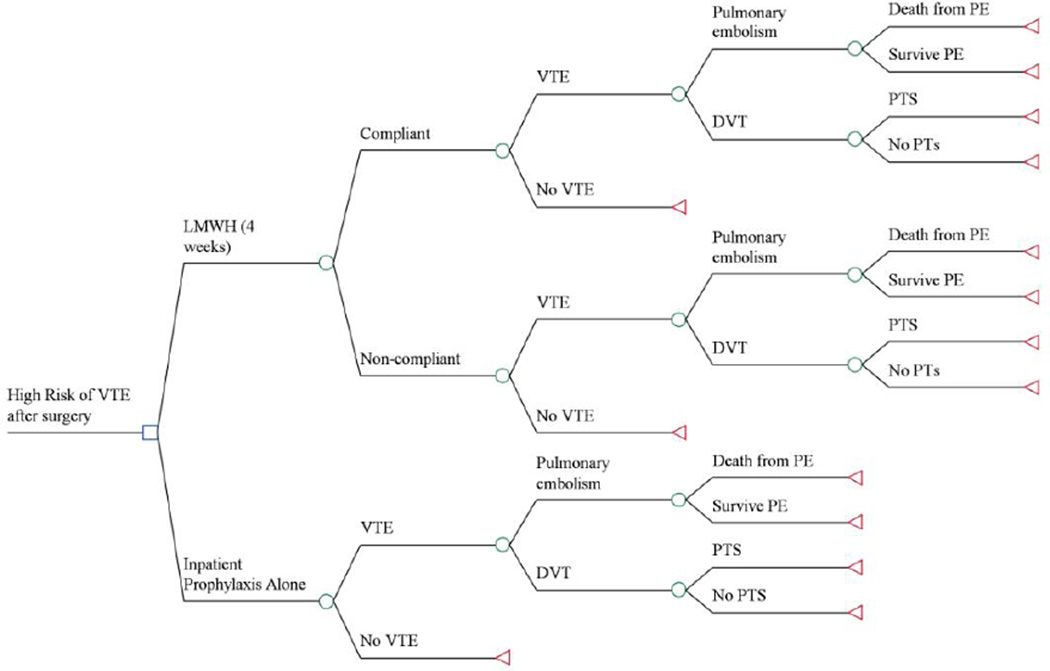
Methods: A decision tree was used to compare EDTPPX for 21 days after discharge to 7 days of inpatient prophylaxis with base case assumptions based on an abdominal oncologic resection without complications in an otherwise healthy individual. Willingness to pay was set at $50,000/quality-adjusted life year (QALY). Sensitivity analyses were performed to assess uncertainty within the model, with particular interest in the threshold for cost-effectiveness based on VTE incidence.
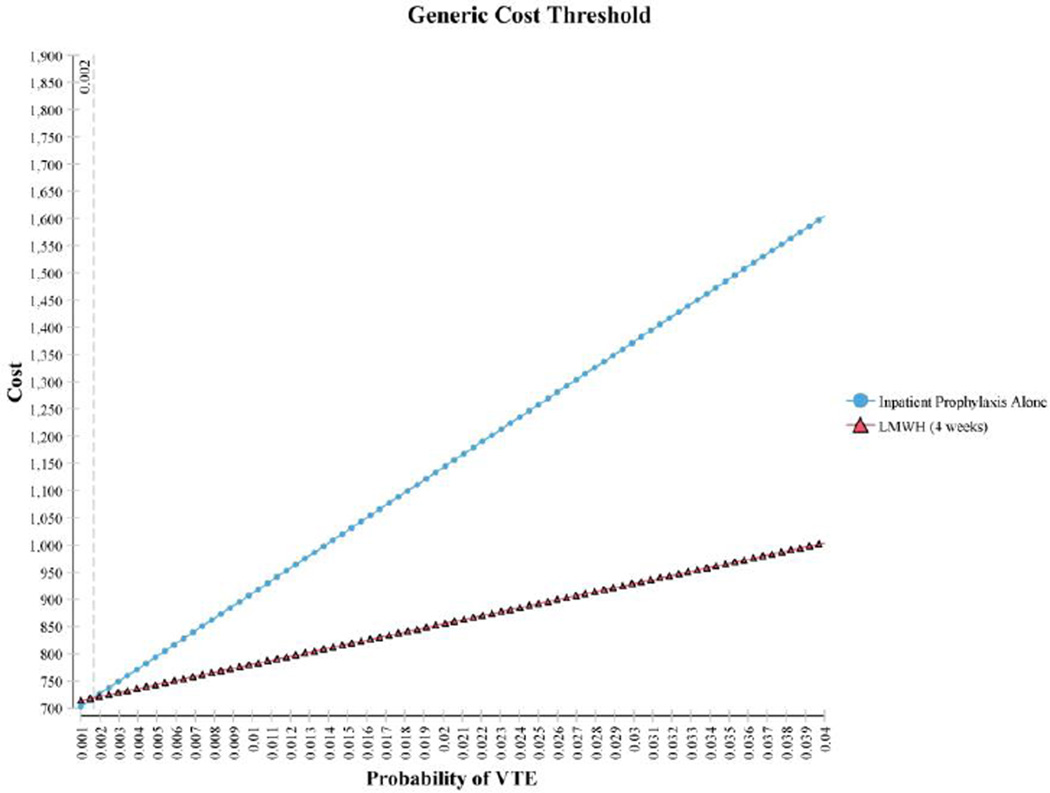
Results: EDTPPX was the dominant strategy when VTE probability exceeds 2.39 %. Given a willingness to pay threshold of $50,000/QALY, EDTPPX was the preferred strategy when VTE incidence exceeded 1.22 and 0.88 % when using brand name or generic medication costs, respectively.
Conclusions: EDTPPX should be recommended whenever VTE incidence exceeds 2.39 %. When post-discharge estimated VTE risk is 0.88-2.39 %, patient preferences about self-injections and medication costs should be considered.
Figures



Similar articles
-
Cost-effectiveness analysis of doctor-pharmacist collaborative prescribing for venous thromboembolism in high risk surgical patients.BMC Health Serv Res. 2018 Oct 1;18(1):749. doi: 10.1186/s12913-018-3557-0. BMC Health Serv Res. 2018. PMID: 30285744 Free PMC article.
-
Extended thromboprophylaxis with low-molecular-weight heparins after hospital discharge in high-risk surgical and medical patients: a review.Clin Ther. 2009 Jun;31(6):1129-41. doi: 10.1016/j.clinthera.2009.06.002. Clin Ther. 2009. PMID: 19695383 Review.
-
A decision model to estimate a risk threshold for venous thromboembolism prophylaxis in hospitalized medical patients.J Thromb Haemost. 2017 Jun;15(6):1132-1141. doi: 10.1111/jth.13687. Epub 2017 May 3. J Thromb Haemost. 2017. PMID: 28371250 Free PMC article.
-
A cost-utility analysis of dabigatran, enoxaparin, and usual care for venous thromboprophylaxis after hip or knee replacement surgery in Thailand.J Thromb Thrombolysis. 2017 Feb;43(2):252-262. doi: 10.1007/s11239-016-1433-5. J Thromb Thrombolysis. 2017. PMID: 27704332
-
The effectiveness of graduated compression stockings for prevention of venous thromboembolism in orthopedic and abdominal surgery patients requiring extended pharmacologic thromboprophylaxis.J Vasc Surg Venous Lymphat Disord. 2018 Nov;6(6):766-777.e2. doi: 10.1016/j.jvsv.2018.05.020. Epub 2018 Aug 17. J Vasc Surg Venous Lymphat Disord. 2018. PMID: 30126797
Cited by
-
Development and validation of a risk calculator for post-discharge venous thromboembolism following hepatectomy for malignancy.HPB (Oxford). 2021 May;23(5):723-732. doi: 10.1016/j.hpb.2020.09.008. Epub 2020 Sep 26. HPB (Oxford). 2021. PMID: 32988755 Free PMC article.
-
Cost-effectiveness of Venous Thromboembolism Prophylaxis After Hospitalization in Patients With Inflammatory Bowel Disease.Inflamm Bowel Dis. 2022 Aug 1;28(8):1169-1176. doi: 10.1093/ibd/izab246. Inflamm Bowel Dis. 2022. PMID: 34591970 Free PMC article.
-
Risk adjusted venous thromboembolism prophylaxis following pancreatic surgery.J Thromb Thrombolysis. 2023 May;55(4):604-616. doi: 10.1007/s11239-023-02775-0. Epub 2023 Jan 25. J Thromb Thrombolysis. 2023. PMID: 36696020
-
Extended venous thromboembolism prophylaxis after abdominopelvic cancer surgery: a retrospective review.Curr Oncol. 2019 Feb;26(1):e106-e110. doi: 10.3747/co.26.4339. Epub 2019 Feb 1. Curr Oncol. 2019. PMID: 30853816 Free PMC article.
-
Post-discharge venous thromboembolism after pancreatectomy for malignancy: Predicting risk based on preoperative, intraoperative, and postoperative factors.J Surg Oncol. 2020 Sep;122(4):675-683. doi: 10.1002/jso.26046. Epub 2020 Jun 12. J Surg Oncol. 2020. PMID: 32531819 Free PMC article.
References
-
- Galson SK. The Surgeon General's Call to Action to Prevent Deep Vein Thrombosis and Pulmonary Embolism. 2008 - PubMed
-
- Anderson FA, Jr, Zayaruzny M, Heit JA, Fidan D, Cohen AT. Estimated annual numbers of US acute-care hospital patients at risk for venous thromboembolism. Am J Hematol. 2007;82(9):777–782. - PubMed
-
- Lausen I, Jensen R, Jorgensen LN, et al. Incidence and prevention of deep venous thrombosis occurring late after general surgery: randomised controlled study of prolonged thromboprophylaxis. Eur J Surg. 1998;164(9):657–663. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
