

Obesity increases length of stay and direct medical costs in total hip arthroplasty
- PMID: 24101527
- PMCID: PMC3940745
- DOI: 10.1007/s11999-013-3316-9
Obesity increases length of stay and direct medical costs in total hip arthroplasty
Abstract
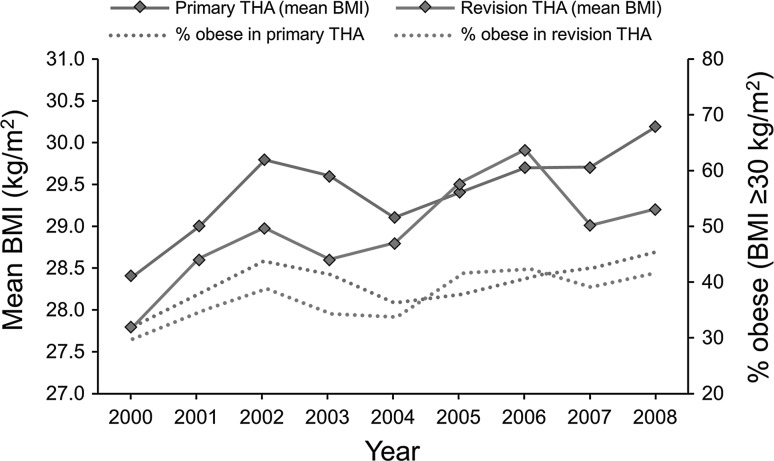
Background: The number of obese patients undergoing THA is increasing. Previous studies have shown that obesity is associated with an increased likelihood of complications after THA, but there is little information regarding the impact of obesity on medical resource use and direct medical costs in THA.
Questions/purposes: We sought to examine the relationship between obesity, length of stay, and direct medical costs in a large cohort of patients undergoing THAs.
Methods: The study included 8973 patients who had undergone 6410 primary and 2563 revision THAs at a large US medical center between January 1, 2000, and September 31, 2008. Patients with bilateral procedures within 90 days after index admission and patients with acute trauma were excluded. Data regarding clinical, surgical characteristics, and complications were obtained from the original medical records and the institutional joint registry. Patients were classified into eight groups based on their BMI at the time of surgery. Direct medical costs were calculated by using standardized, inflation-adjusted costs for services and procedures billed during hospitalization and the 90-day window. Study end points were hospital length of stay, direct medical costs during hospitalization, and the 90-day window. End points were compared across the eight BMI categories in multivariable risk-adjusted linear regression models.
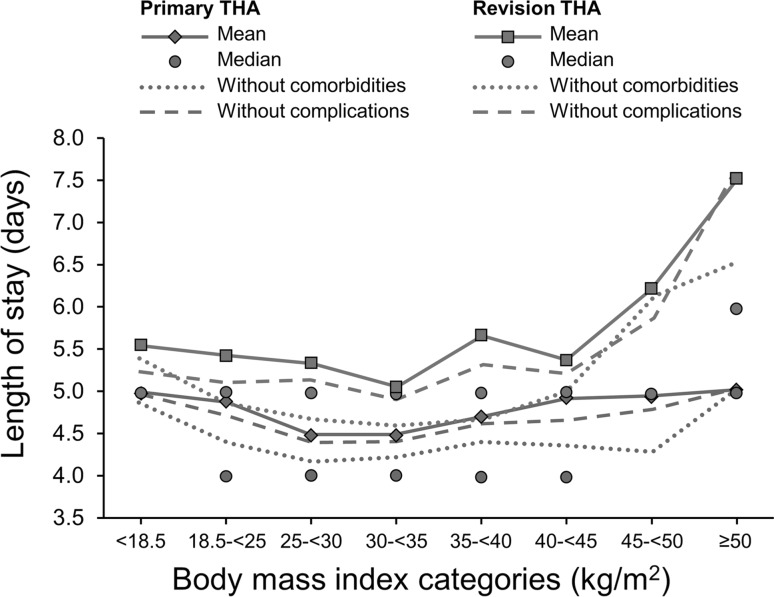
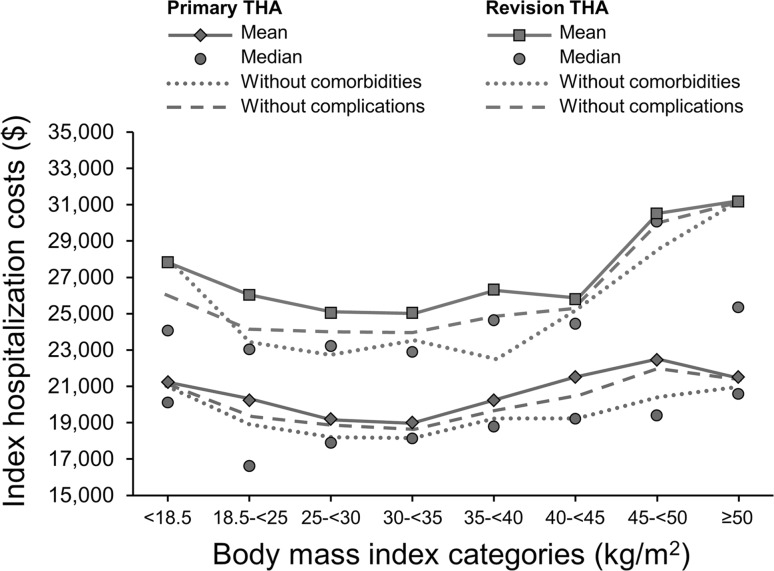
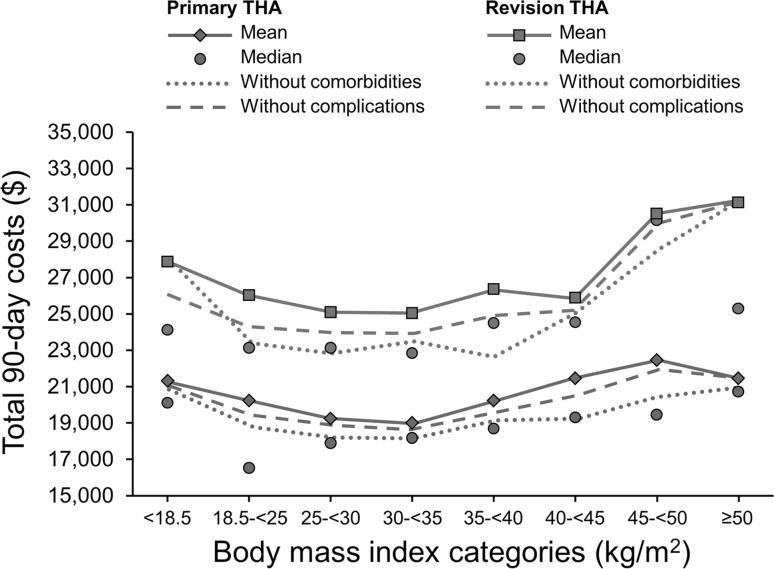
Results: Mean length of stay and the direct medical costs were lowest for patients with a BMI of 25 to 35 kg/m(2). Increasing BMI was associated with longer hospital stays and costs. Every five-unit increase in BMI beyond 30 kg/m(2) was associated with approximately USD $500 higher hospital costs and USD $900 higher 90-day costs in primary THA (p = 0.0001), which corresponded to 5% higher costs. The cost increase associated with BMI was greater in the revision THA cohort where every five-unit increase in BMI beyond 30 kg/m(2) was associated with approximately USD $800 higher hospital costs and USD $1500 higher 90-day costs. These estimates remained unchanged after adjusting for comorbidities or complications.
Conclusions: Obesity is associated with longer hospital stays and higher costs in THA. The significant effect of obesity on costs persists even among patients without comorbidities but the increased costs associated with obesity may be balanced by the potential benefits of THA in the obese. Increasing prevalence of obesity likely contributes to the increasing financial burden of THA worldwide.
Level of evidence: Level IV, economic and decision analyses. See the Instructions for Authors for a complete description of levels of evidence.
Figures
Similar articles
-
The effect of obesity on direct medical costs in total knee arthroplasty.J Bone Joint Surg Am. 2014 May 7;96(9):718-24. doi: 10.2106/JBJS.M.00819. J Bone Joint Surg Am. 2014. PMID: 24806008
-
Hospital costs of total hip arthroplasty for developmental dysplasia of the hip.Clin Orthop Relat Res. 2014 Jul;472(7):2237-44. doi: 10.1007/s11999-014-3587-9. Epub 2014 Apr 11. Clin Orthop Relat Res. 2014. PMID: 24723141 Free PMC article.
-
Comparative Epidemiology of Revision Arthroplasty: Failed THA Poses Greater Clinical and Economic Burdens Than Failed TKA.Clin Orthop Relat Res. 2015 Jun;473(6):2131-8. doi: 10.1007/s11999-014-4078-8. Epub 2014 Dec 3. Clin Orthop Relat Res. 2015. PMID: 25467789 Free PMC article.
-
Factors associated with hospital stay length, discharge destination, and 30-day readmission rate after primary hip or knee arthroplasty: Retrospective Cohort Study.Orthop Traumatol Surg Res. 2019 Sep;105(5):949-955. doi: 10.1016/j.otsr.2019.04.012. Epub 2019 Jun 15. Orthop Traumatol Surg Res. 2019. PMID: 31208932 Review.
-
Economic costs of adult obesity: a review of recent European studies with a focus on subgroup-specific costs.Maturitas. 2011 Jul;69(3):220-9. doi: 10.1016/j.maturitas.2011.04.005. Epub 2011 May 18. Maturitas. 2011. PMID: 21592692 Review.
Cited by
-
Total Hip Arthroplasty in the Obese Patient: Tips and Tricks and Review of the Literature.Indian J Orthop. 2020 Jun 10;54(6):776-783. doi: 10.1007/s43465-020-00164-w. eCollection 2020 Nov. Indian J Orthop. 2020. PMID: 33133400 Free PMC article. Review.
-
Factors Associated With 30-Day Readmission After Primary Total Hip Arthroplasty: Analysis of 514 455 Procedures in the UK National Health Service.JAMA Surg. 2017 Dec 20;152(12):e173949. doi: 10.1001/jamasurg.2017.3949. Epub 2017 Dec 20. JAMA Surg. 2017. PMID: 28979994 Free PMC article.
-
Limited Influence of Comorbidities on Length of Stay after Total Hip Arthroplasty: Experience of Enhanced Recovery after Surgery.Orthop Surg. 2020 Feb;12(1):153-161. doi: 10.1111/os.12600. Epub 2019 Dec 29. Orthop Surg. 2020. PMID: 31885219 Free PMC article.
-
Length of stay and its impact upon functional outcomes following lower limb arthroplasty.Knee Surg Sports Traumatol Arthrosc. 2017 Sep;25(9):2676-2681. doi: 10.1007/s00167-015-3914-z. Epub 2015 Dec 30. Knee Surg Sports Traumatol Arthrosc. 2017. PMID: 26718640
-
Economic analysis of two-stage septic revision after total hip arthroplasty: What are the relevant costs for the hospital's orthopedic department?BMC Musculoskelet Disord. 2016 Mar 1;17:112. doi: 10.1186/s12891-016-0962-6. BMC Musculoskelet Disord. 2016. PMID: 26932453 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
