

Enhancement of vasoreactivity and cognition by intranasal insulin in type 2 diabetes
- PMID: 24101698
- PMCID: PMC3931384
- DOI: 10.2337/dc13-1672
Enhancement of vasoreactivity and cognition by intranasal insulin in type 2 diabetes
Abstract
Objective: To determine acute effects of intranasal insulin on regional cerebral perfusion and cognition in older adults with type 2 diabetes mellitus (DM).
Research design and methods: This was a proof-of-concept, randomized, double-blind, placebo-controlled intervention evaluating the effects of a single 40-IU dose of insulin or saline on vasoreactivity and cognition in 15 DM and 14 control subjects. Measurements included regional perfusion, vasodilatation to hypercapnia with 3-Tesla MRI, and neuropsychological evaluation.
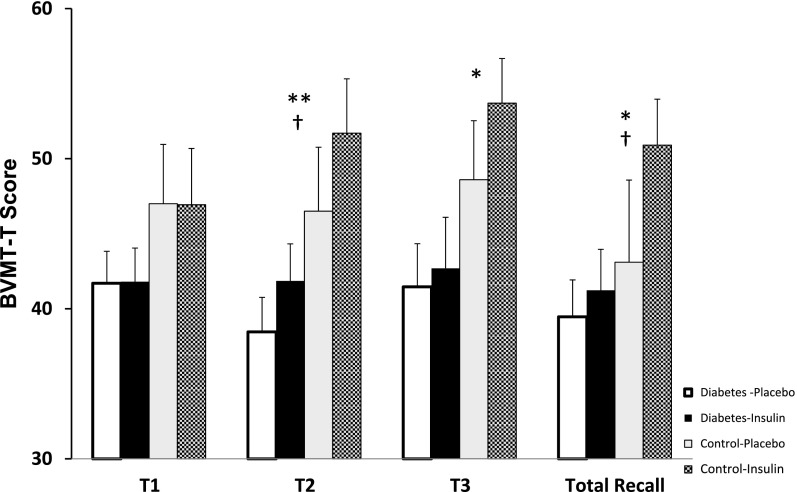
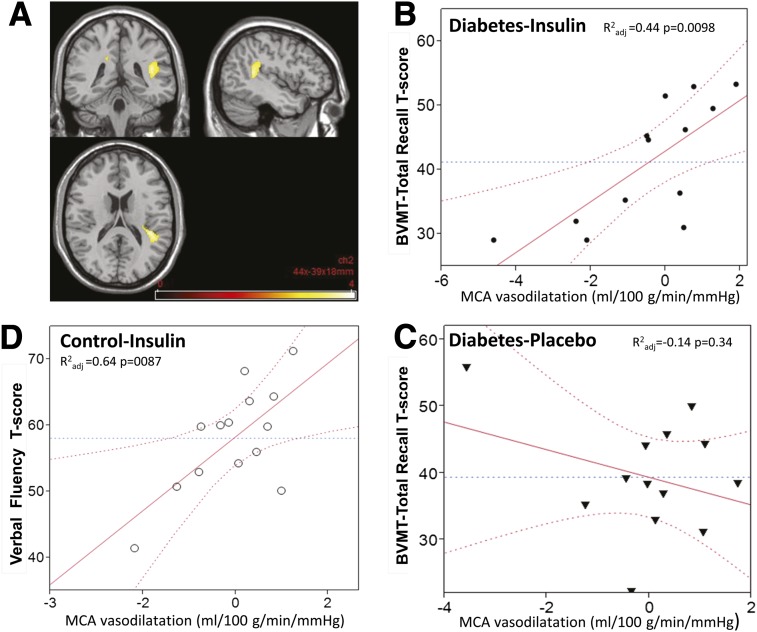
Results: Intranasal insulin administration was well tolerated and did not affect systemic glucose levels. No serious adverse events were reported. Across all subjects, intranasal insulin improved visuospatial memory (P ≤ 0.05). In the DM group, an increase of perfusion after insulin administration was greater in the insular cortex compared with the control group (P = 0.0003). Cognitive performance after insulin administration was related to regional vasoreactivity. Improvements of visuospatial memory after insulin administration in the DM group (R(2)adjusted = 0.44, P = 0.0098) and in the verbal fluency test in the control group (R(2)adjusted = 0.64, P = 0.0087) were correlated with vasodilatation in the middle cerebral artery territory.
Conclusions: Intranasal insulin administration appears safe, does not affect systemic glucose control, and may provide acute improvements of cognitive function in patients with type 2 DM, potentially through vasoreactivity mechanisms. Intranasal insulin-induced changes in cognitive function may be related to vasodilatation in the anterior brain regions, such as insular cortex that regulates attention-related task performance. Larger studies are warranted to identify long-term effects and predictors of positive cognitive response to intranasal insulin therapy.
Trial registration: ClinicalTrials.gov NCT01206322.
Figures
References
-
- Xu WL, Qiu CX, Wahlin A, Winblad B, Fratiglioni L. Diabetes mellitus and risk of dementia in the Kungsholmen project: a 6-year follow-up study. Neurology 2004;63:1181–1186 - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- 8UL1TR000170-05/TR/NCATS NIH HHS/United States
- 8KL2TR000168-05/TR/NCATS NIH HHS/United States
- P50 AG005136/AG/NIA NIH HHS/United States
- R21 DK084463/DK/NIDDK NIH HHS/United States
- UL1 TR000170/TR/NCATS NIH HHS/United States
- R01 AG027415/AG/NIA NIH HHS/United States
- KL2 RR025757/RR/NCRR NIH HHS/United States
- 5R21-DK-084463-02/DK/NIDDK NIH HHS/United States
- KL2 TR000168/TR/NCATS NIH HHS/United States
- 1R01-AG-0287601-A2/AG/NIA NIH HHS/United States
- 1KL2RR025757-04/RR/NCRR NIH HHS/United States
- R01-AG-027415/AG/NIA NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
