

Superior sulcus (Pancoast) tumors: current evidence on diagnosis and radical treatment
- PMID: 24102007
- PMCID: PMC3791502
- DOI: 10.3978/j.issn.2072-1439.2013.04.08
Superior sulcus (Pancoast) tumors: current evidence on diagnosis and radical treatment
Abstract
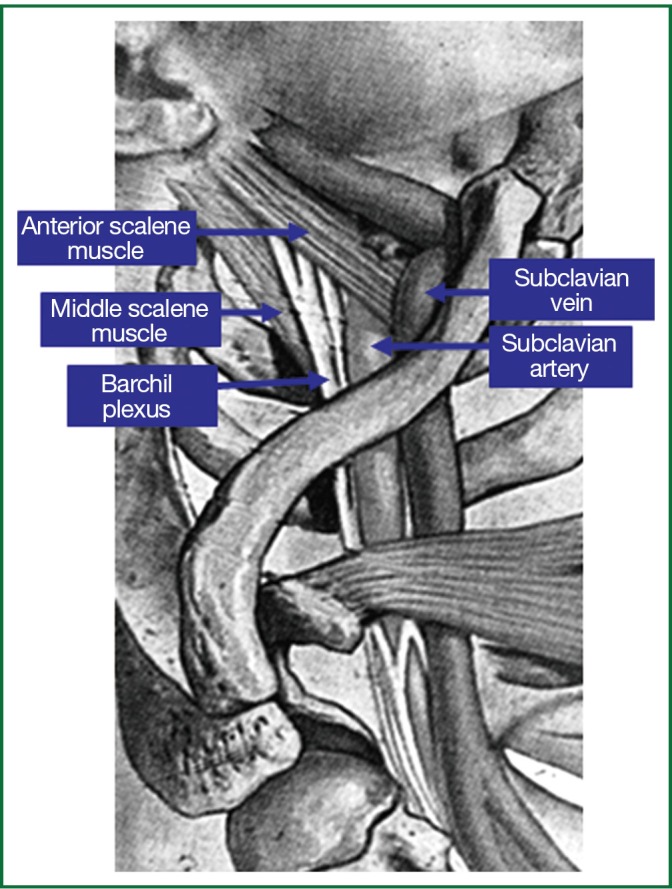
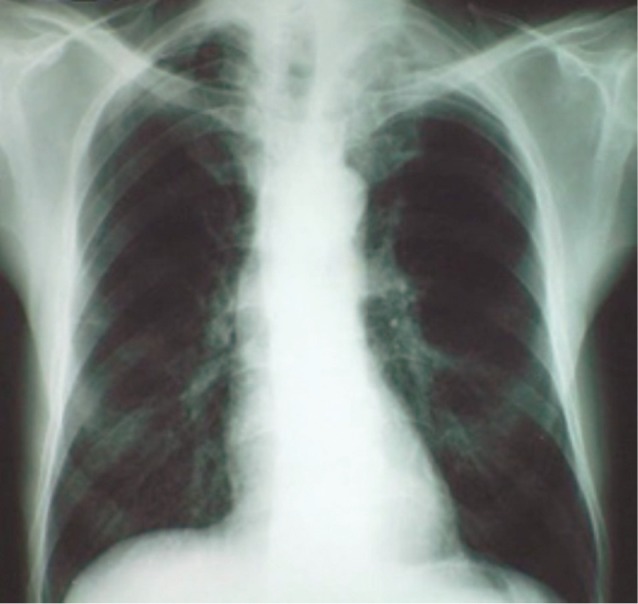
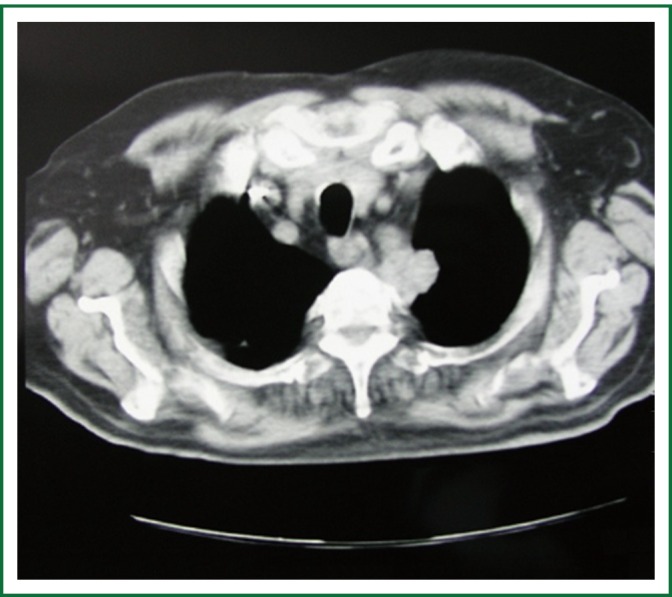
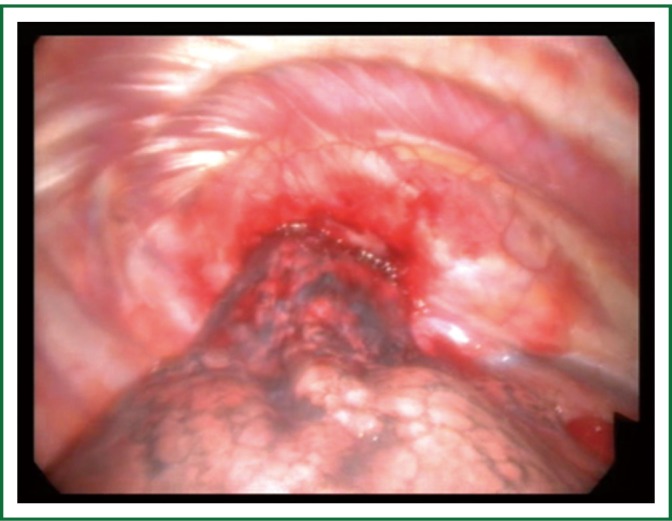
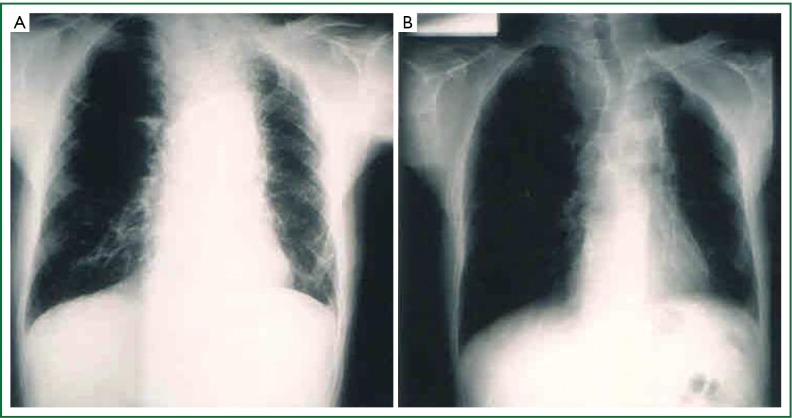
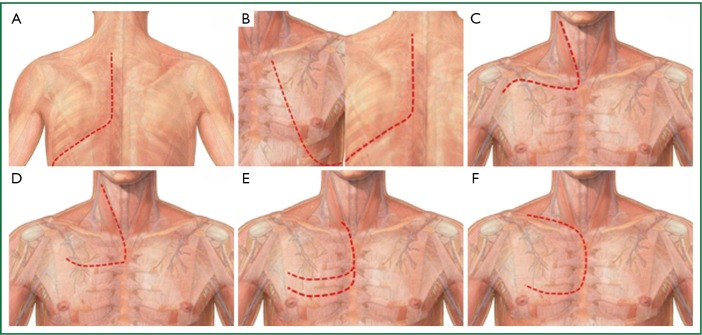
Pancoast tumors account for less than 5% of all bronchogenic carcinomas. These tumors are located in the apex of the lung and involve through tissue contiguity the apical chest wall and/or the structures of the thoracic inlet. The tumors become clinically evident with the characteristic symptoms of the "Pancoast-Tobias syndrome" which includes Claude-Bernard-Horner syndrome, severe pain in the shoulder radiating toward the axilla and/or scapula and along the ulnar distribution of the upper arm, atrophy of hand and arm muscles and obstruction of the subclavian vein resulting in edema of the upper arm. The diagnosis will be made by the combination of the characteristic clinical symptoms with the radiographic findings of a mass or opacity in the apex of the lung infiltrating the 1(st) and/or 2(nd) ribs. A tissue diagnosis of the tumor via CT-guided FNA/B should always be available before the initiation of treatment. Bronchoscopy, thoracoscopy and biopsy of palpable supraclavicular nodes are alternative ways to obtain a tissue diagnosis. Adenocarcinomas account for 2/3 of all Pancoast tumors, while the rest of the tumors are squamous cell and large cell carcinomas. Magnetic resonance imaging of the thoracic inlet is always recommended to define the exact extent of tumor invasion within the thoracic inlet before surgical intervention. Pancoast tumors are by definition T3 or T4 tumors. Induction chemo-radiotherapy is the standard of care for any potentially resectable Pancoast tumor followed by an attempt to achieve a complete tumor resection. Resection can be made through a variety of anterior and posterior approaches to the thoracic inlet. The choice of the approach depends on the location of the tumor (posterior - middle - anterior compartment of the thoracic inlet) and the depth/extent of invasion. Prognosis depends mainly on T stage of tumor, response to preoperative chemo-radiotherapy and completeness of resection. Resection of the invaded strictures of the thoracic inlet should me made en bloc with pulmonary parenchyma resection, preferably an upper lobectomy. Invasion of the vertebral column is not a contraindication for surgery which, however, should be performed in oncologic centers with experience in spinal surgery. Surgery for Pancoast tumors is associated with 5% mortality rate and the complication rate varies from 7-38%. The overall 2-year survival rate after induction chemo-radiotherapy and resection varies from 55% to 70%, while the 5-year survival for R0 resections is quite good (54-77%). The main pattern of recurrence is that of distant metastases, especially in the brain.
Keywords: Pancoast; lung cancer; treatment.
Figures
References
-
- Arcasoy SM, Jett JR. Superior pulmonary sulcus tumors and Pancoast’s syndrome. N Engl J Med 1997;337:1370-6 - PubMed
-
- Pitz CC, de la Rivière AB, van Swieten HA, et al. Surgical treatment of Pancoast tumours. Eur J Cardiothorac Surg 2004;26:202-8 - PubMed
-
- Detterbeck FC. Changes in the treatment of Pancoast tumors. Ann Thorac Surg 2003;75:1990-7 - PubMed
-
- Shen KR, Meyers BF, Larner JM, et al. Special treatment issues in lung cancer: ACCP evidence-based clinical practice guidelines (2nd edition). Chest 2007;132:290S-305S. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous