

Accuracy of diagnostic biopsy for cutaneous melanoma: implications for surgical oncologists
- PMID: 24102023
- PMCID: PMC3786502
- DOI: 10.1155/2013/196493
Accuracy of diagnostic biopsy for cutaneous melanoma: implications for surgical oncologists
Abstract
Background and objectives: While excisional biopsy is recommended to diagnose cutaneous melanoma, various biopsy techniques are used in practice. We undertook this study to identify how frequently final tumor stage and treatment recommendations changed from diagnostic biopsy to final histopathology after wide local excision (WLE).
Methods: We compared the histopathology of the dermatopathologist-reviewed diagnostic biopsy and final WLE in 332 cutaneous melanoma patients.
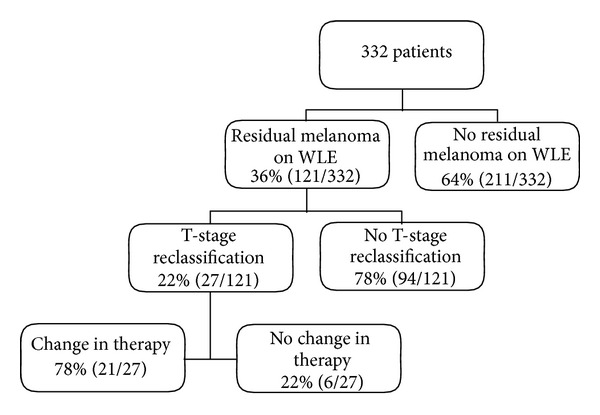
Results: Tumor sites were extremity (51%), trunk (33%), and head/neck (16%). Initial biopsy types were excisional (56%), punch (21%), shave (18%), and incisional (5%). Most diagnostic biopsies were margin positive regardless of technique, and 36% of patients had residual melanoma on WLE. T-stage changed in 8% of patients, of whom 59% were diagnosed by punch biopsy, 15% by incisional biopsy, 15% by shave biopsy, and 11% by excisional biopsy (P < 0.0001). Treatment recommendations changed in 6%: 2% after excisional biopsy, 5% after shave biopsy, 18% after punch biopsy, and 18% after incisional biopsy (P < 0.0001).
Conclusions: Although most biopsy margins were positive, T-stage and treatment changed for only a minority of melanoma patients. Our data provide valuable information to inform patient discussion regarding the likelihood of a change in prognosis and the need for secondary procedures after WLE. These data support the superiority of dermatopathologist-reviewed excisional biopsy when feasible.
Figures
Similar articles
-
Effect of biopsy type on outcomes in the treatment of primary cutaneous melanoma.Am J Surg. 2013 May;205(5):585-90; discussion 590. doi: 10.1016/j.amjsurg.2013.01.023. Am J Surg. 2013. PMID: 23592167
-
Accuracy of partial biopsies in the management of cutaneous melanoma.Australas J Dermatol. 2019 Aug;60(3):209-213. doi: 10.1111/ajd.13004. Epub 2019 Feb 17. Australas J Dermatol. 2019. PMID: 30773625
-
Clinical Impact and Accuracy of Shave Biopsy for Initial Diagnosis of Cutaneous Melanoma.J Surg Res. 2023 Jun;286:35-40. doi: 10.1016/j.jss.2022.12.042. Epub 2023 Feb 3. J Surg Res. 2023. PMID: 36739830
-
Skin Biopsy Techniques.Prim Care. 2022 Mar;49(1):1-22. doi: 10.1016/j.pop.2021.10.001. Epub 2022 Jan 5. Prim Care. 2022. PMID: 35125151 Review.
-
Role of In Vivo Reflectance Confocal Microscopy in the Analysis of Melanocytic Lesions.Acta Dermatovenerol Croat. 2018 Apr;26(1):64-67. Acta Dermatovenerol Croat. 2018. PMID: 29782304 Review.
Cited by
-
Impact of Biopsy Technique on Clinically Important Outcomes for Cutaneous Melanoma: A Systematic Review and Meta-analysis.Mayo Clin Proc Innov Qual Outcomes. 2020 Jul 15;4(4):373-383. doi: 10.1016/j.mayocpiqo.2020.04.005. eCollection 2020 Aug. Mayo Clin Proc Innov Qual Outcomes. 2020. PMID: 32793865 Free PMC article. Review.
-
Effect of changes in Breslow thickness between the initial punch biopsy results and final pathology reports in acral lentiginous melanoma patients.Sci Rep. 2021 Oct 6;11(1):19885. doi: 10.1038/s41598-021-99422-6. Sci Rep. 2021. PMID: 34615974 Free PMC article.
-
Impact of Shave Biopsy on Diagnosis and Management of Cutaneous Melanoma: A Systematic Review and Meta-Analysis.Ann Surg Oncol. 2021 Oct;28(11):6168-6176. doi: 10.1245/s10434-021-09866-3. Epub 2021 Mar 29. Ann Surg Oncol. 2021. PMID: 33782802 Free PMC article.
-
Diagnostic biopsy of cutaneous melanoma, sentinel lymph node biopsy and indications for lymphadenectomy.World J Clin Oncol. 2022 Oct 24;13(10):861-865. doi: 10.5306/wjco.v13.i10.861. World J Clin Oncol. 2022. PMID: 36337309 Free PMC article.
-
Preoperative measurement of cutaneous melanoma and nevi thickness with photoacoustic imaging.J Med Imaging (Bellingham). 2018 Jan;5(1):015004. doi: 10.1117/1.JMI.5.1.015004. Epub 2018 Feb 13. J Med Imaging (Bellingham). 2018. PMID: 29487881 Free PMC article.
References
-
- Siegel R, Naishadham D, Jemal A. Cancer statistics, 2013. CA Cancer Journal for Clinicians. 2013;63(2):11–30. - PubMed
-
- Ho VC, Milton GW, Sober AJ. Biopsy of melanoma. In: Balch C, editor. Cutaneous Melanoma. 2nd edition. Philadelphia, Pa, USA: JB Lippincott; 1992. pp. 264–268.
-
- Bishop JAN, Corrie PG, Hall PN, et al. UK guidelines for the management of cutaneous melanoma. British Journal of Plastic Surgery. 2002;55(1):46–54. - PubMed
-
- Australian Cancer Network Melanoma Guidelines Revision Working Party. Clinical Practice Guidelines For the Management of Melanoma in Australia and New Zealand. Wellington, New Zealand: The Cancer Council Australia, Australian Cancer Network; 2008. Biopsy; pp. 35–39. (Sydney and New Zealand Guidelines Group).
-
- NCCN Clinical Practice Guidelines in Oncology: Melanoma V. 4. 2011. http://www.nccn.org/, 2011.
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
