

Intracerebral hemorrhage and delirium symptoms. Length of stay, function, and quality of life in a 114-patient cohort
- PMID: 24102675
- PMCID: PMC3919076
- DOI: 10.1164/rccm.201307-1256OC
Intracerebral hemorrhage and delirium symptoms. Length of stay, function, and quality of life in a 114-patient cohort
Abstract
Rationale: The prognostic significance of delirium symptoms in intensive care unit (ICU) patients with focal neurologic injury is unclear.
Objectives: To determine the relationship between delirium symptoms and subsequent functional outcomes and quality of life (QOL) after intracerebral hemorrhage.
Methods: We prospectively enrolled 114 patients. Delirium symptoms were routinely assessed twice daily using the Confusion Assessment Method for the ICU by trained nurses. Functional outcomes were recorded with modified Rankin Scale (scored from 0 [no symptoms] to 6 [dead]), and QOL outcomes with Neuro-QOL at 28 days, 3 months, and 12 months.
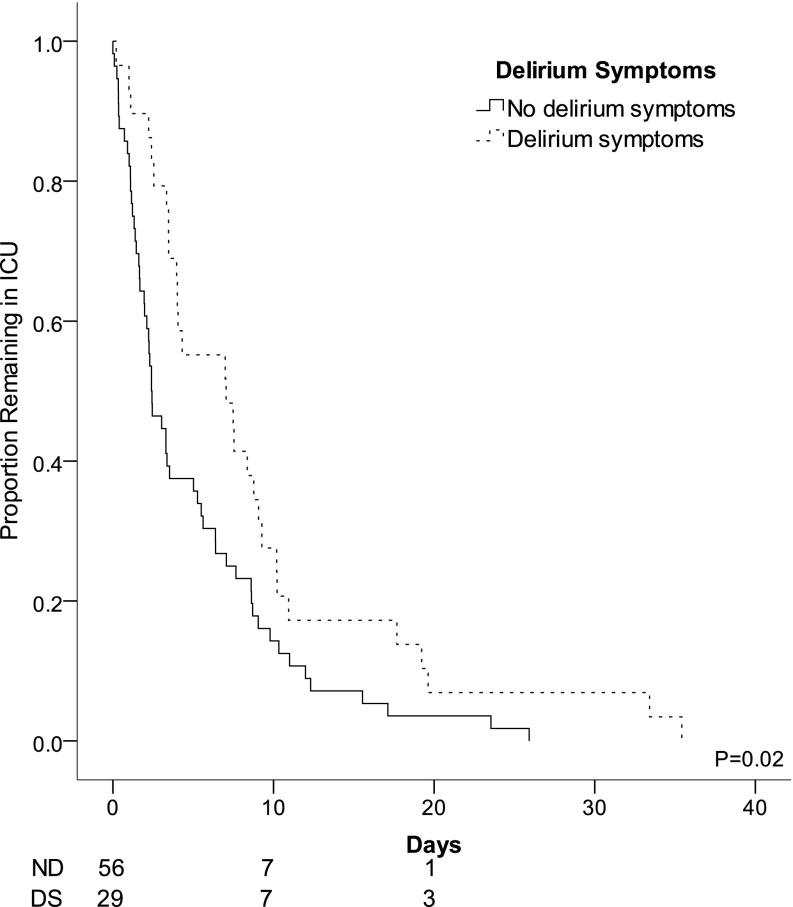
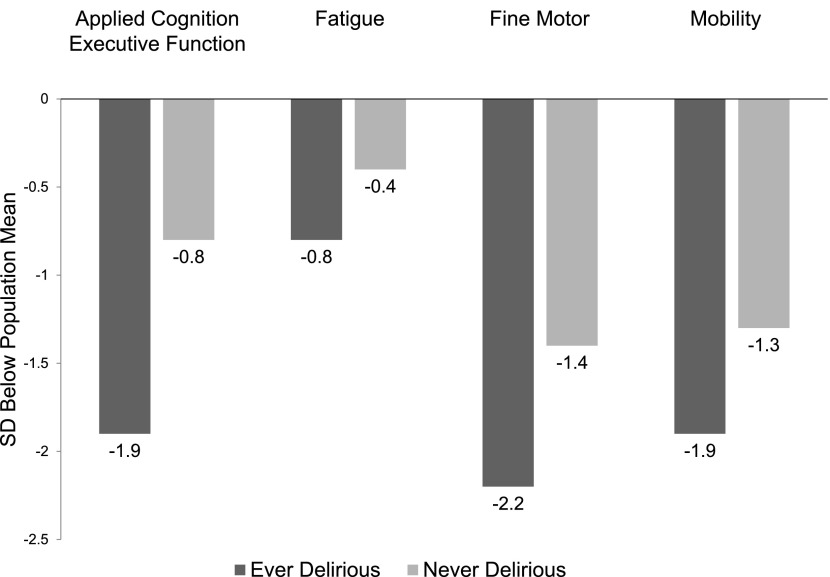
Measurements and main results: Thirty-one (27%) patients had delirium symptoms ("ever delirious"), 67 (59%) were never delirious, and the remainder (14%) had persistent coma. Delirium symptoms were nearly always hypoactive, were detected mean 6 days after intracerebral hemorrhage presentation, and were associated with longer ICU length of stay (mean 3.5 d longer in ever vs. never delirious patients; 95% confidence interval, 1.5-8.3; P = 0.004) after correction for age, admit National Institutes of Health (NIH) Stroke Scale, and any benzodiazepine exposure. Delirium symptoms were associated with increased odds of poor outcome at 28 days (odds ratio, 8.7; 95% confidence interval, 1.4-52.5; P = 0.018) after correction for admission NIH Stroke Scale and age, and with worse QOL in the domains of applied cognition-executive function and fatigue after correcting for the NIH Stroke Scale, age, benzodiazepine exposure, and time of follow-up.
Conclusions: After focal neurologic injury, delirium symptoms were common despite low rates of infection and sedation exposure, and were predictive of subsequent worse functional outcomes and lower QOL.
Figures
Comment in
-
Studying outcomes that matter to patients and families: quality of life after intracerebral hemorrhage.Am J Respir Crit Care Med. 2013 Dec 1;188(11):1278-9. doi: 10.1164/rccm.201310-1836ED. Am J Respir Crit Care Med. 2013. PMID: 24289770 No abstract available.
References
-
- Ely EW, Shintani A, Truman B, Speroff T, Gordon SM, Harrell FE, Jr, Inouye SK, Bernard GR, Dittus RS. Delirium as a predictor of mortality in mechanically ventilated patients in the intensive care unit. JAMA. 2004;291:1753–1762. - PubMed
-
- Lin SM, Huang CD, Liu CY, Lin HC, Wang CH, Huang PY, Fang YF, Shieh MH, Kuo HP. Risk factors for the development of early-onset delirium and the subsequent clinical outcome in mechanically ventilated patients. J Crit Care. 2008;23:372–379. - PubMed
-
- Pandharipande PP, Pun BT, Herr DL, Maze M, Girard TD, Miller RR, Shintani AK, Thompson JL, Jackson JC, Deppen SA, et al. Effect of sedation with dexmedetomidine vs lorazepam on acute brain dysfunction in mechanically ventilated patients: the MENDS randomized controlled trial. JAMA. 2007;298:2644–2653. - PubMed
-
- Pandharipande P, Shintani A, Peterson J, Pun BT, Wilkinson GR, Dittus RS, Bernard GR, Ely EW. Lorazepam is an independent risk factor for transitioning to delirium in intensive care unit patients. Anesthesiology. 2006;104:21–26. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
