

Controversies in timing of dialysis initiation and the role of race and demographics
- PMID: 24102770
- PMCID: PMC3836868
- DOI: 10.1111/sdi.12130
Controversies in timing of dialysis initiation and the role of race and demographics
Abstract
Dialysis remains the predominant form of renal replacement therapy in the United States, but the optimal timing for the initiation of dialysis remains poorly defined. Not only clinical factors such as signs/symptoms of uremia, co-existing cardiovascular disease, and presence of diabetes but also key demographic characteristics including age, gender, race/ethnicity, and socioeconomics have all been considered as potential modifying factors in the decision for the timing of dialysis initiation. The 2012 Kidney Disease: Improving Global Outcomes (KDIGO) Clinical Practice Guideline for the Evaluation and Management of chronic kidney disease (CKD) suggests that dialysis be initiated when signs/symptoms attributable to kidney failure such as serositis, acid-base or electrolyte abnormalities, pruritus, poorly controlled volume status or blood pressure, deteriorating nutritional status despite dietary intervention, or cognitive impairment are visible or noted. These signs/symptoms typically occur when the glomerular filtration rate (GFR) is in the range of 5-10 ml/minute/1.73 m(2) , although they may occur at higher levels of GFR. We review recent data on the timing of dialysis initiation, their implications for managing patients with late-stage CKD, and the important role of considering key demographics in making patient-centered decisions for the timing of dialysis initiation.
© 2013 Wiley Periodicals, Inc.
Conflict of interest statement
None declared.
Figures
Similar articles
-
Late initiation of dialysis among women and ethnic minorities in the United States.J Am Soc Nephrol. 2000 Dec;11(12):2351-2357. doi: 10.1681/ASN.V11122351. J Am Soc Nephrol. 2000. PMID: 11095658
-
Provider and care characteristics associated with timing of dialysis initiation.Clin J Am Soc Nephrol. 2014 Feb;9(2):310-7. doi: 10.2215/CJN.04190413. Epub 2014 Jan 16. Clin J Am Soc Nephrol. 2014. PMID: 24436477 Free PMC article.
-
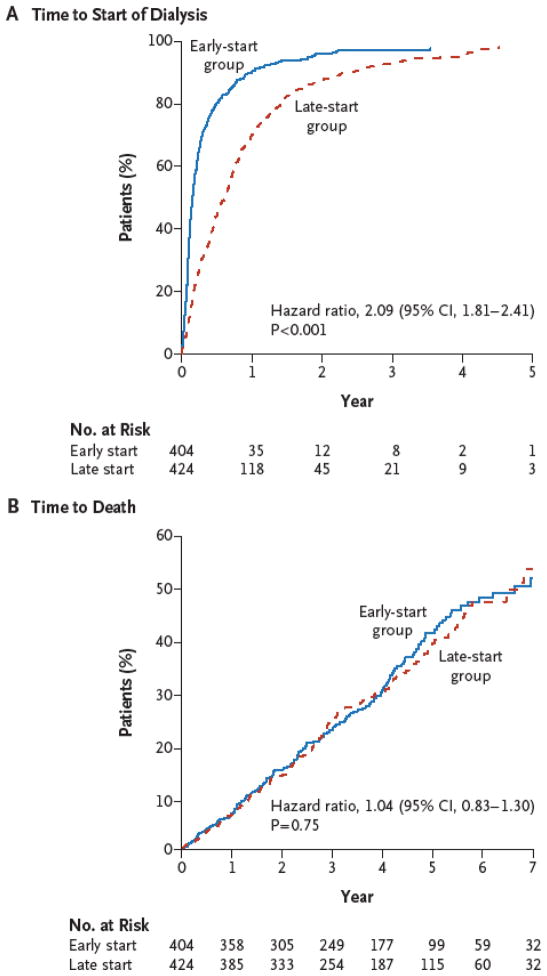
A randomized, controlled trial of early versus late initiation of dialysis.N Engl J Med. 2010 Aug 12;363(7):609-19. doi: 10.1056/NEJMoa1000552. Epub 2010 Jun 27. N Engl J Med. 2010. PMID: 20581422 Clinical Trial.
-
Update of dialysis initiation timing in end stage kidney disease patients: is it a resolved question? A systematic literature review.BMC Nephrol. 2023 Jun 7;24(1):162. doi: 10.1186/s12882-023-03184-4. BMC Nephrol. 2023. PMID: 37286965 Free PMC article.
-
Initiation of dialysis should be timely: neither early nor late.Semin Dial. 2013 Nov-Dec;26(6):644-9. doi: 10.1111/sdi.12127. Epub 2013 Sep 4. Semin Dial. 2013. PMID: 24004413 Review.
Cited by
-
Geographic Dialysis Facility Density and Early Dialysis Initiation.JAMA Netw Open. 2024 Jan 2;7(1):e2350009. doi: 10.1001/jamanetworkopen.2023.50009. JAMA Netw Open. 2024. PMID: 38170525 Free PMC article.
-
Initiation of Hemodialysis After Eight Years Following the Diagnosis of Stage 5 Chronic Kidney Disease: A Case Report.Cureus. 2020 Nov 6;12(11):e11357. doi: 10.7759/cureus.11357. Cureus. 2020. PMID: 33178542 Free PMC article.
-
The Construction and Meaning of Race Within Hypertension Guidelines: A Systematic Scoping Review.J Gen Intern Med. 2024 Oct;39(13):2531-2542. doi: 10.1007/s11606-024-08874-9. Epub 2024 Jul 1. J Gen Intern Med. 2024. PMID: 38954319 Free PMC article.
-
Explaining trends and variation in timing of dialysis initiation in the United States.Medicine (Baltimore). 2017 May;96(20):e6911. doi: 10.1097/MD.0000000000006911. Medicine (Baltimore). 2017. PMID: 28514305 Free PMC article.
-
From race-based to race-conscious medicine: how anti-racist uprisings call us to act.Lancet. 2020 Oct 10;396(10257):1125-1128. doi: 10.1016/S0140-6736(20)32076-6. Lancet. 2020. PMID: 33038972 Free PMC article. No abstract available.
References
-
- Rosansky S, Glassock RJ, Clark WF. Early start of dialysis: a critical review. Clin J Am Soc Nephrol. 2011;6:1222–1228. - PubMed
-
- Rosansky SJ, Clark WF, Eggers P, Glassock RJ. Initiation of dialysis at higher GFRs: is the apparent rising tide of early dialysis harmful or helpful? Kidney Int. 2009;76:257–261. - PubMed
-
- Obrador GT, Pereira BJ. Early referral to the nephrologist and timely initiation of renal replacement therapy: a paradigm shift in the management of patients with chronic renal failure. Am J Kidney Dis. 1998;31:398–417. - PubMed
-
- Liu H, Peng Y, Liu F, Xiao H, Chen X, Huang A, Liu Y. Renal function and serum albumin at the start of dialysis in 514 Chinese ESRD in-patients. Ren Fail. 2008;30:685–690. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
