

Relationships between the intention to use guidelines, behaviour of insurance physicians and their determinants
- PMID: 24103198
- PMCID: PMC3851955
- DOI: 10.1186/1472-6963-13-400
Relationships between the intention to use guidelines, behaviour of insurance physicians and their determinants
Abstract
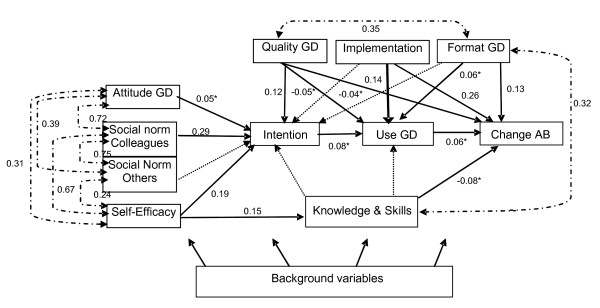
Background: We studied the intention of a group of insurance physicians to use the guidelines for depression, and their behaviour in disability assessments. We considered attitude, social norm and self-efficacy, knowledge/skills and stimuli, based on the Attitude-Social norm-self-Efficacy model (ASE model) as possible determinants of both intention and behaviour.The aim of this study was to understand the determinants of insurance physicians' behaviour when they are expected to use guidelines in daily practice.
Method: A representative sample of 42 insurance physicians participated in this study. Cross-sectional data were collected by means of a questionnaire based on the ASE model. We developed the questionnaire on the basis of literature and ascertained the content validity of it. Behaviour was made to comprise both "use of the guidelines" and "change in disability assessment behaviour" by the insurance physicians. Reliability analyses were performed to form additive scales of the ASE constructs. These scales were analysed with structural equations modelling (LISREL), by modifying a start model into a final model with a good fit, within theoretical constraints. In these analyses special attention was paid to the fact that the sample size was small.
Results: The most important determinants of the intention and the self-reported use of the guidelines, were: the influence of colleagues, the self-efficacy of the insurance physicians in their use of the guidelines, and the way the guidelines were implemented. The intention to use the guidelines for depression was not associated with the self-reported use of these guidelines, but there proved to be a faint, positive association with the self-reported change in assessment behaviour.
Conclusions: Almost all the insurance physicians in this study intended to use at least elements of the guidelines. Their intention, self reported use of the guidelines and self-reported change in assessment behaviour were explored with help of the ASE model. The model suggested relationships between intention, self reported use of the guidelines and self-reported change in assessment behaviour on the on the one hand and various determinants on the other hand. Be that as it may, we see opportunities to improve insurance physicians' guideline adherence by offering them a multifaceted training in which they learn to apply the guidelines for depression.
Figures



Similar articles
-
Changes in insurance physicians' attitudes, self-efficacy, intention, and knowledge and skills regarding the guidelines for depression, following an implementation strategy.J Occup Rehabil. 2013 Mar;23(1):148-56. doi: 10.1007/s10926-012-9378-9. J Occup Rehabil. 2013. PMID: 22763493 Free PMC article. Clinical Trial.
-
Can self-reported disability assessment behaviour of insurance physicians be explained? Applying the ASE model.BMC Public Health. 2011 Jul 19;11:576. doi: 10.1186/1471-2458-11-576. BMC Public Health. 2011. PMID: 21771326 Free PMC article.
-
The development of instruments to measure the work disability assessment behaviour of insurance physicians.BMC Public Health. 2011 Jan 3;11:1. doi: 10.1186/1471-2458-11-1. BMC Public Health. 2011. PMID: 21199570 Free PMC article.
-
Determinants of physicians' communication behaviour in disability assessments.Disabil Rehabil. 2011;33(13-14):1157-68. doi: 10.3109/09638288.2010.524269. Epub 2010 Oct 19. Disabil Rehabil. 2011. PMID: 20958178
-
Determinants of compliance with infection prevention measures by physicians: a scoping review.J Hosp Infect. 2024 Nov;153:30-38. doi: 10.1016/j.jhin.2024.08.011. Epub 2024 Aug 28. J Hosp Infect. 2024. PMID: 39214255
Cited by
-
Examination of psychosocial predictors of Chinese hospital pharmacists' intention to provide clinical pharmacy services using the theory of planned behaviour: a cross-sectional questionnaire study.BMJ Open. 2016 Oct 5;6(10):e012775. doi: 10.1136/bmjopen-2016-012775. BMJ Open. 2016. PMID: 27707835 Free PMC article.
-
Use of theory to plan or evaluate guideline implementation among physicians: a scoping review.Implement Sci. 2017 Feb 27;12(1):26. doi: 10.1186/s13012-017-0557-0. Implement Sci. 2017. PMID: 28241771 Free PMC article.
-
Changes in insurance physicians' attitudes, self-efficacy, intention, and knowledge and skills regarding the guidelines for depression, following an implementation strategy.J Occup Rehabil. 2013 Mar;23(1):148-56. doi: 10.1007/s10926-012-9378-9. J Occup Rehabil. 2013. PMID: 22763493 Free PMC article. Clinical Trial.
-
Prevention and Management of Obesity in Children with Autism Spectrum Disorder Among Primary Care Pediatricians.J Autism Dev Disord. 2018 Jul;48(7):2408-2417. doi: 10.1007/s10803-018-3494-0. J Autism Dev Disord. 2018. PMID: 29450838 Free PMC article.
References
-
- Grol R, Wensing M. What drives change? Barriers to and incentives for achieving evidence-based practice. Med J Aust. 2004;180(6 Suppl):S57–S60. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
