

Analytical validation of the Oncotype DX prostate cancer assay - a clinical RT-PCR assay optimized for prostate needle biopsies
- PMID: 24103217
- PMCID: PMC4007703
- DOI: 10.1186/1471-2164-14-690
Analytical validation of the Oncotype DX prostate cancer assay - a clinical RT-PCR assay optimized for prostate needle biopsies
Abstract
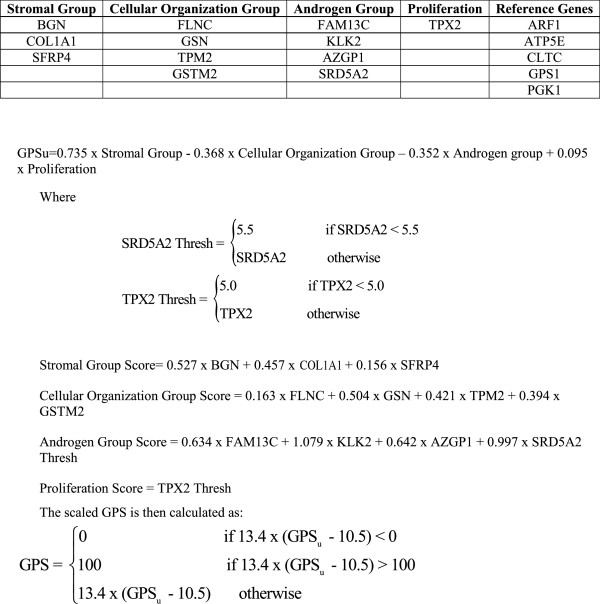
Background: The Oncotype DX Prostate Cancer Assay is a multi-gene RT-PCR expression assay that was developed for use with fixed paraffin-embedded (FPE) diagnostic prostate needle biopsies containing as little as 1 mm of prostate tumor in the greatest dimension. The assay measures expression of 12 cancer-related genes representing four biological pathways and 5 reference genes which are algorithmically combined to calculate the Genomic Prostate Score (GPS). This biopsy-based assay has been analytically and subsequently clinically validated as a predictor of aggressive prostate cancer. The aim of this study was to validate the analytical performance of the Oncotype DX Prostate Cancer Assay using predefined acceptance criteria.
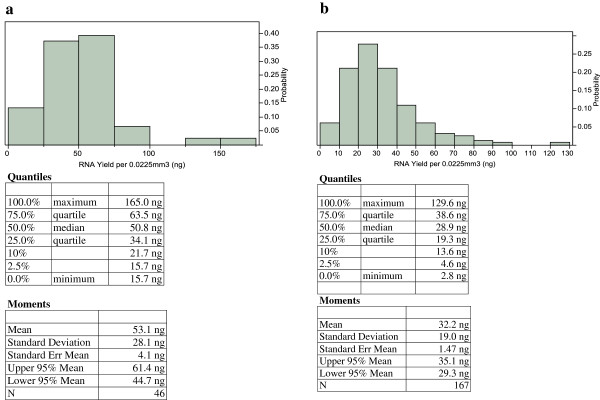
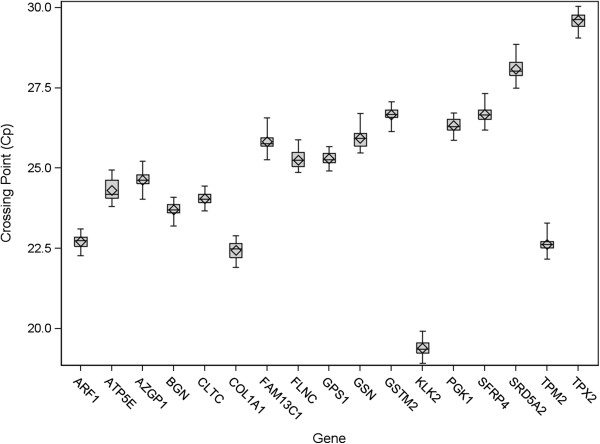
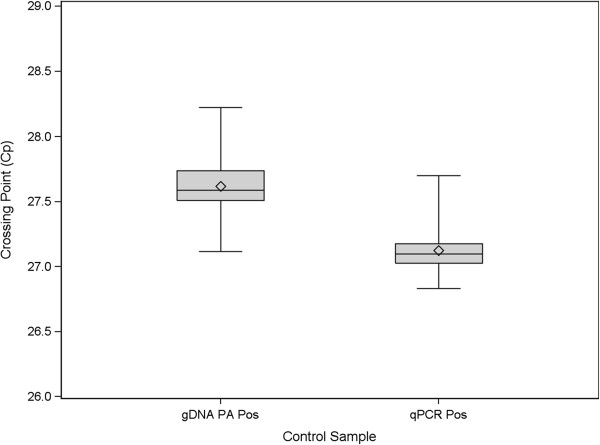
Results: The lowest quartile of RNA yields from prostate needle biopsies (six 5 μm sections) was between 19 and 34 ng. Analytical validation of the process requiring as little as 5 ng of RNA met all pre-defined acceptance criteria. Amplification efficiencies, analytical sensitivity, and accuracy of gene assays were measured by serially diluting an RNA sample and analyzing features of the linear regression between RNA expression measured by the crossing point (Cp) versus the log2 of the RNA input per PCR assay well. Gene assays were shown to accurately measure expression over a wide range of inputs (from as low as 0.005 ng to 320 ng). Analytical accuracy was excellent with average biases at qPCR inputs representative of patient samples <9.7% across all assays while amplification efficiencies were within ±6% of the median. Assessments of reproducibility and precision were performed by testing 10 prostate cancer RNA samples over multiple instruments, reagent lots, operators, days (precision), and RNA input levels (reproducibility) using appropriately parameterized linear mixed models. The standard deviations for analytical precision and reproducibility were 1.86 and 2.11 GPS units (100-unit scale) respectively.
Conclusions: The Oncotype DX Prostate Cancer Assay, a clinical RT-PCR assay specifically designed for use with prostate needle biopsies, has been analytically validated using very limited RNA inputs. The assay requirements and analytical performance will provide physicians with test results from a robust and reliable assay which will enable improved treatment decisions for men diagnosed with early-stage prostate cancer.
Figures
References
-
- Teutsch SM, Bradley LA, Palomaki GE, Haddow JE, Piper M, Calonge N, Dotson WD, Douglas MP, Berg AO, Group EW. The Evaluation of Genomic Applications in Practice and Prevention (EGAPP) Initiative: methods of the EGAPP Working Group. Genet Med. 2009;14(1):3–14. doi: 10.1097/GIM.0b013e318184137c. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
