

The effect of adherence to ACLS protocols on survival of event in the setting of in-hospital cardiac arrest
- PMID: 24103233
- PMCID: PMC3886248
- DOI: 10.1016/j.resuscitation.2013.09.019
The effect of adherence to ACLS protocols on survival of event in the setting of in-hospital cardiac arrest
Abstract
Aim: Advanced Cardiac Life Support (ACLS) algorithms are the default standard of care for in-hospital cardiac arrest (IHCA) management. However, adherence to published guidelines is relatively poor. The records of 149 patients who experienced IHCA were examined to begin to understand the association between overall adherence to ACLS protocols and successful return of spontaneous circulation (ROSC).
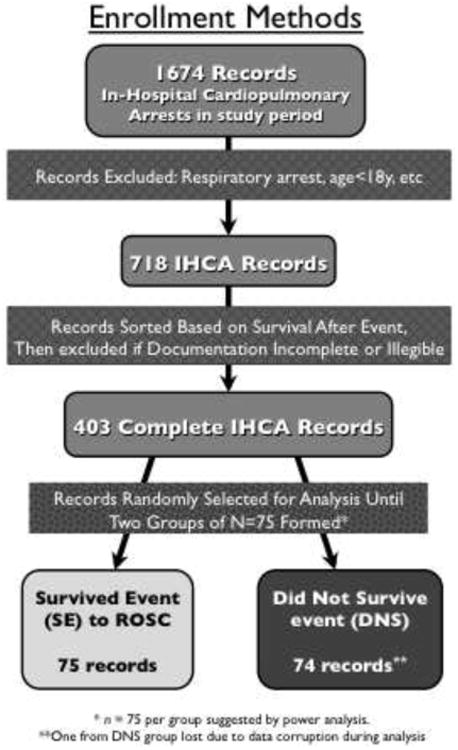
Methods: A retrospective chart review of medical records and code team worksheets was conducted for 75 patients who had ROSC after an IHCA event (SE group) and 74 who did not survive an IHCA event (DNS group). Protocol adherence was assessed using a detailed checklist based on the 2005 ACLS Update protocols. Several additional patient characteristics and circumstances were also examined as potential predictors of ROSC.
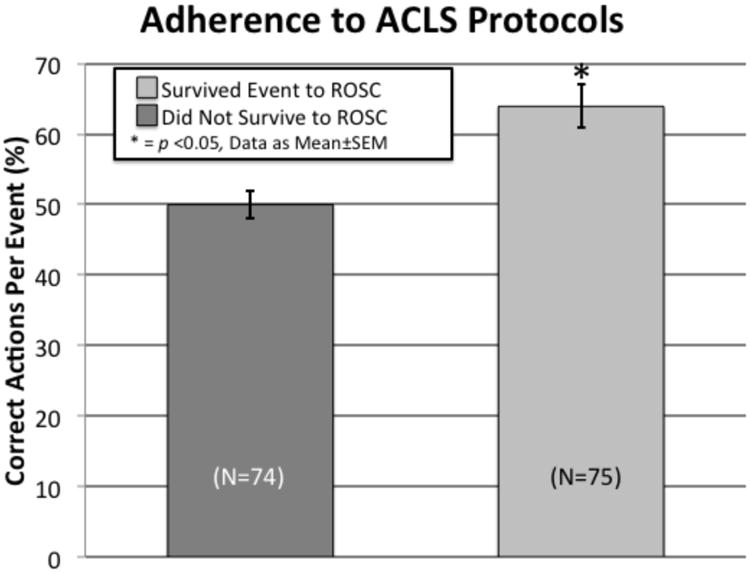
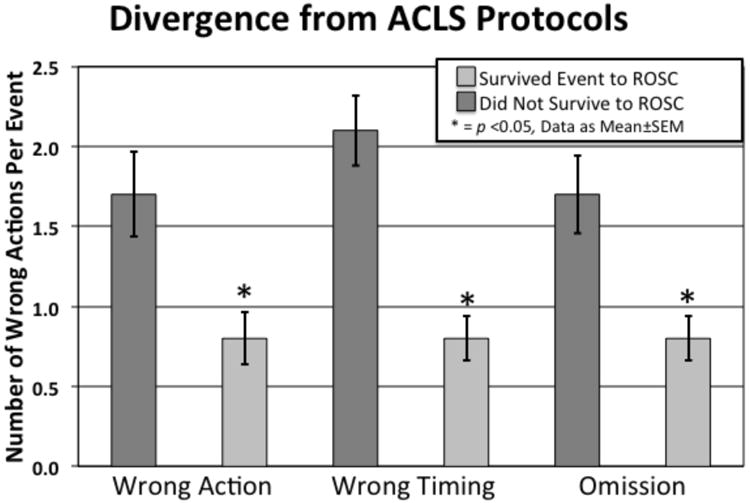
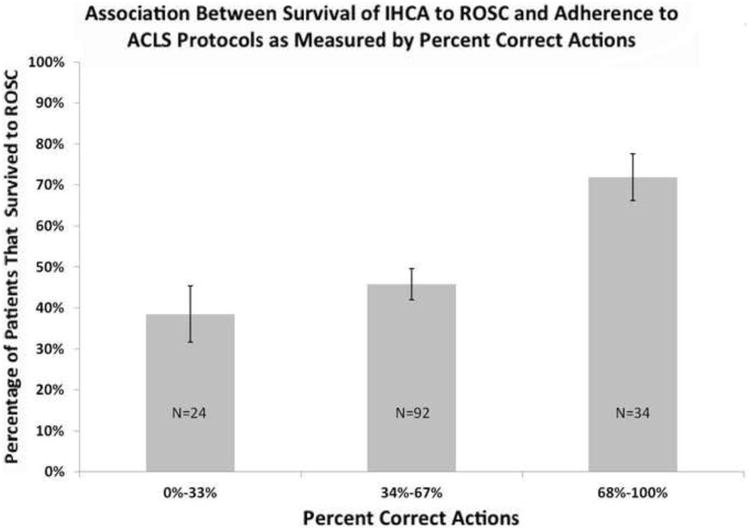
Results: In unadjusted analyses, the percentage of correct steps performed was positively correlated with ROSC from an IHCA (p<0.01), and the number of errors of commission and omission were both negatively correlated with ROSC from an IHCA (p<0.01). In multivariable models, the percentage of correct steps performed and the number of errors of commission and omission remained significantly predictive of ROSC (p<0.01 and p<0.0001, respectively) even after accounting for confounders such as the difference in age and location of the IHCAs.
Conclusions: Our results show that adherence to ACLS protocols throughout an event is correlated with increased ROSC in the setting of cardiac arrest. Furthermore, the results suggest that, in addition to correct actions, both wrong actions and omissions of indicated actions lead to decreased ROSC after IHCA.
Keywords: Advanced Cardiac Life Support; In-hospital cardiac arrest; Protocol adherence; Quality outcomes; Return of spontaneous circulation.
Copyright © 2013 Elsevier Ireland Ltd. All rights reserved.
Conflict of interest statement
Figures

References
-
- Danciu SC, Klein L, Hosseini MM, Ibrahim L, Coyle BW, Kehoe RF. A predictive model for survival after in-hospital cardiopulmonary arrest. Resuscitation. 2004;62:35–42. - PubMed
-
- Moretti MA, Cesar LA, Nusbacher A, Kern KB, Timerman S, Ramires JA. Advanced cardiac life support training improves long-term survival from in-hospital cardiac arrest. Resuscitation. 2007;72:458–65. - PubMed
-
- Silber JH, Kennedy SK, Even-Shoshan O, et al. Anesthesiologist direction and patient outcomes. Anesthesiology. 2000;93:152–63. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
