

Psychosis in Alzheimer's disease
- PMID: 24103379
- PMCID: PMC4036443
- DOI: 10.1016/j.biopsych.2013.08.020
Psychosis in Alzheimer's disease
Abstract
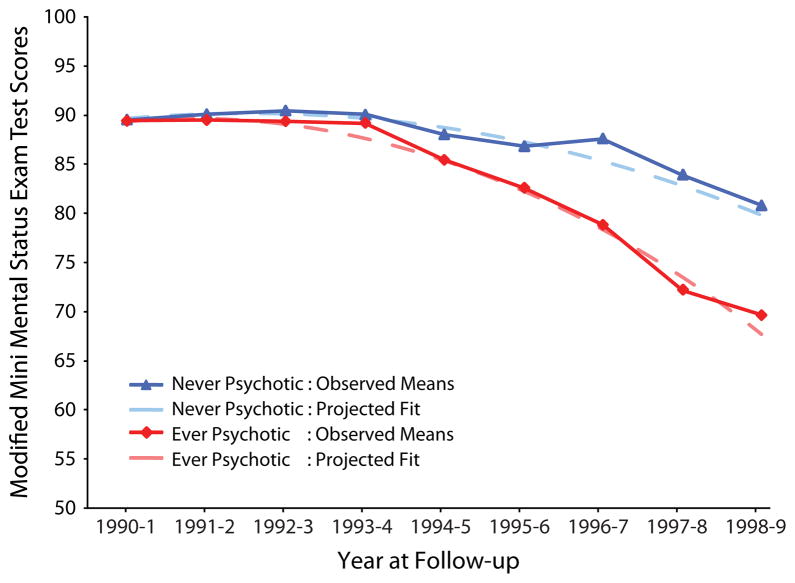
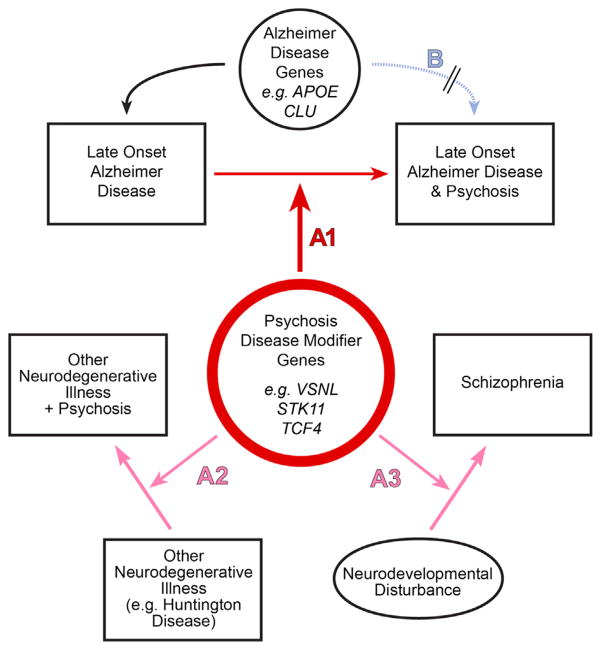
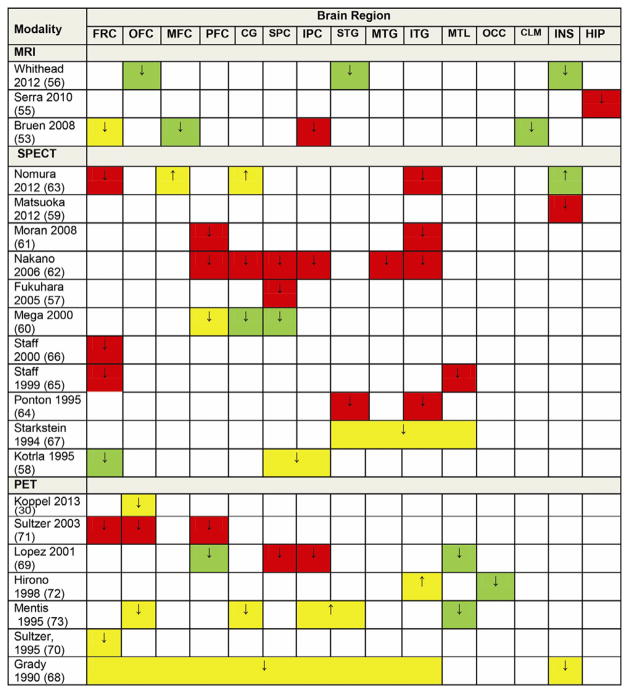
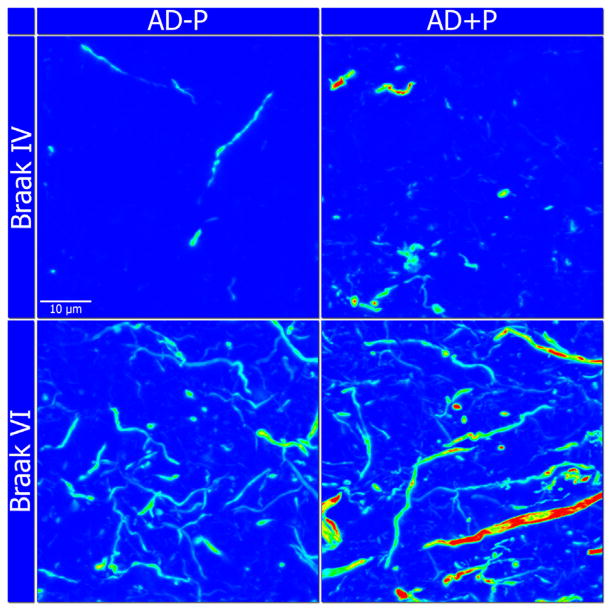
Psychotic symptoms, delusions and hallucinations, occur in approximately 50% of individuals with Alzheimer's disease (AD) (AD with psychosis [AD + P]). Pharmacotherapies for AD + P have limited efficacy and can increase short-term mortality. These observations have motivated efforts to identify the underlying biology of AD + P. Psychosis in AD indicates a more severe phenotype, with more rapid cognitive decline beginning even before psychosis onset. Neuroimaging studies suggest that AD + P subjects demonstrate greater cortical synaptic impairments than AD subjects without psychosis, reflected in reduced gray matter volume, reduced regional blood flow, and reduced regional glucose metabolism. Neuroimaging and available postmortem evidence further indicate that the impairments in AD + P, relative to AD subjects without psychosis, are localized to neocortex rather than medial temporal lobe. Neuropathologic studies provide consistent evidence of accelerated accumulation of hyperphosphorylated microtubule associated protein tau in AD + P. Finally, studies of familial aggregation of AD + P have established that the risk for psychosis in AD is, in part, genetically mediated. Although no genes are established as associated with AD + P, the first genome-wide association study of AD + P has generated some promising leads. The study of the neurobiology of AD + P is rapidly accelerating and may be poised for translational discovery. This process can be enhanced by identifying points of convergence and divergence with the neurobiology of AD proper and of schizophrenia, by innovative extension of current approaches, and by development of relevant animal models.
Keywords: Alzheimer’s disease; genetics; heritability; neuroimaging; neuropathology; psychosis.
Copyright © 2014 Society of Biological Psychiatry. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Dr. Sweet serves as a consultant for Lilly, USA. Drs. Murray, Kumar, and DeMichele-Sweet report no biomedical financial interests or potential conflicts of interest.
Figures
References
-
- Tariot PN, Mack JL, Patterson MB, Edland SD, Weiner MF, Fillenbaum G, et al. The Behavior Rating Scale for Dementia of the Consortium to Establish a Registry for Alzheimer’s Disease. The Behavioral Pathology Committee of the Consortium to Establish a Registry for Alzheimer’s Disease. Am J Psychiatry. 1995;152:1349–1357. - PubMed
-
- Rubin EH, Drevets WC, Burke WJ. Nature of psychotic symptoms in senile dementia of the Alzheimer type. J Geriatr Psychiatry Neurol. 1988;1:17–20. - PubMed
-
- Jeste DV, Finkel SI. Psychosis of Alzheimer’s disease and related dementias. Am J Geriatr Psychiatry. 2000;8:29–34. - PubMed
-
- Paulsen JS, Salmon DP, Thal L, Romero R, Weisstein-Jenkins C, Galasko D, et al. Incidence of and risk factors for hallucinations and delusions in patients with probable Alzheimer’s disease. Neurology. 2000;54:1965–1971. - PubMed
-
- Wilkosz PA, Miyahara S, Lopez OL, DeKosky ST, Sweet RA. Prediction of psychosis onset in Alzheimer disease: The role of cognitive impairment, depressive symptoms, and further evidence for psychosis subtypes. Am J Geriatr Psychiatry. 2006;14:352–360. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
