

An update on the impact of pre-transplant transfusions and allosensitization on time to renal transplant and on allograft survival
- PMID: 24107093
- PMCID: PMC4125965
- DOI: 10.1186/1471-2369-14-217
An update on the impact of pre-transplant transfusions and allosensitization on time to renal transplant and on allograft survival
Abstract
Background: Blood transfusions have the potential to improve graft survival, induce sensitization, and transmit infections. Current clinical practice is to minimize transfusions in renal transplantation candidates, but it is unclear if the evidence continues to support pre-transplant transfusion avoidance. Changes in the Medicare prospective payment system may increase transfusion rates. Thus there is a need to re-evaluate the literature to improve the management options for renal transplant candidates.
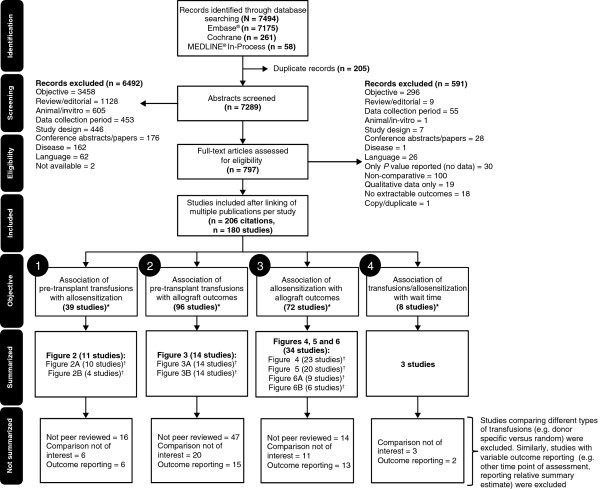
Methods: A review applying a systematic approach and conducted using MEDLINE(®), Embase(®), and the Cochrane Library for English-language publications (timeframe: 01/1984-03/2011) captured 180 studies and data from publically available registries and assessed the impact of transfusions on allosensitization and graft survival, and the impact of allosensitization on graft survival and wait time.
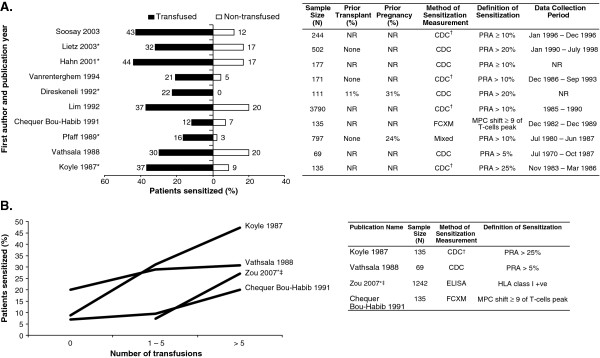
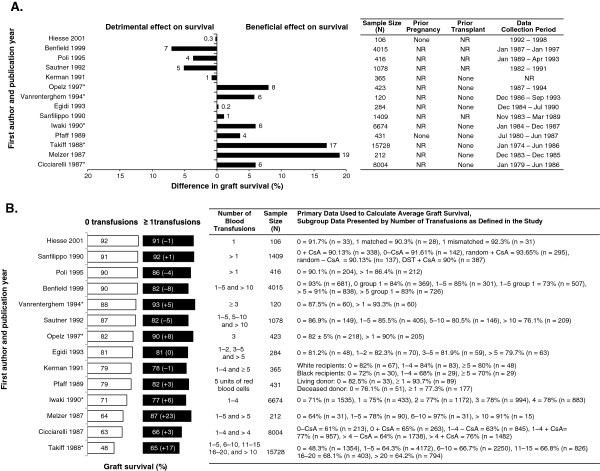
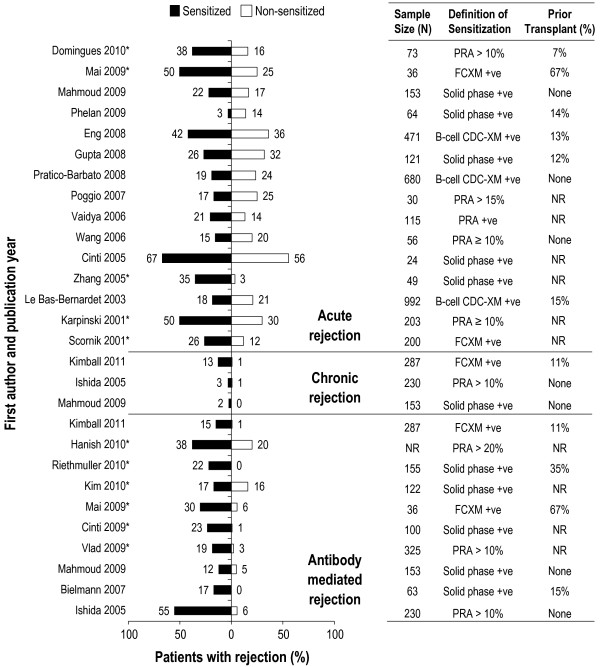
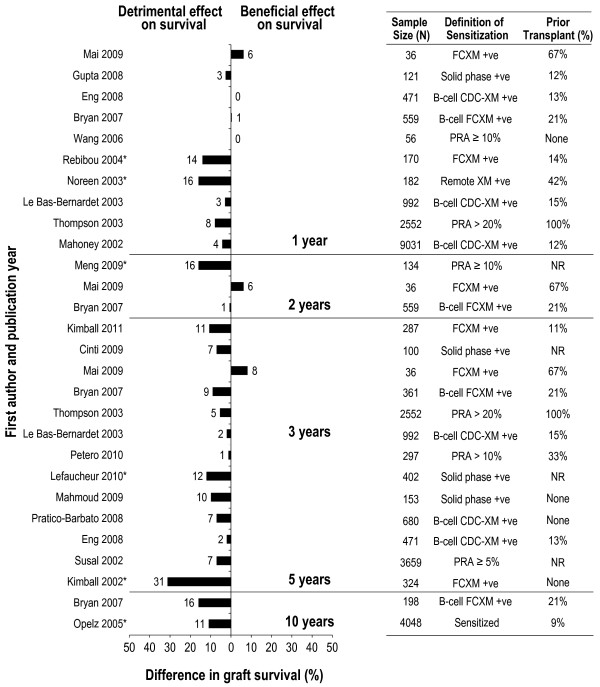
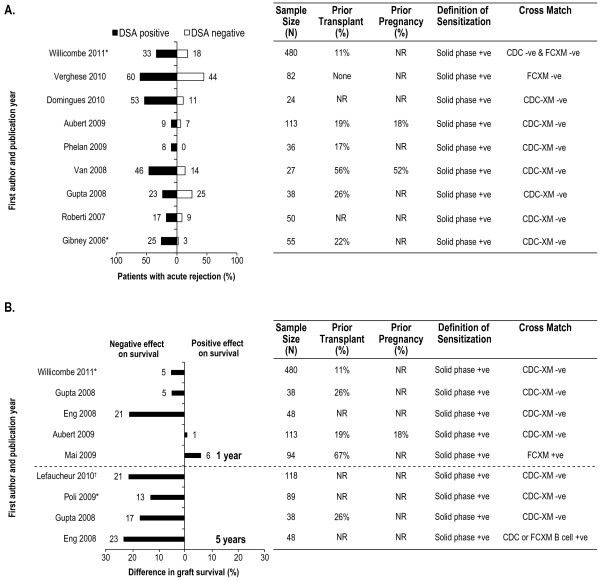
Results: Blood transfusions continued to be a major cause of allosensitization, with allosensitization associated with increased rejection and graft loss, and longer wait times to transplantation. Although older studies showed a beneficial effect of transfusion on graft survival, this benefit has largely disappeared in the post-cyclosporine era due to improved graft outcomes with current practice. Recent data suggested that it may be the donor-specific antibody component of allosensitization that carried the risk to graft outcomes.
Conclusions: Results of this review indicated that avoiding transfusions whenever possible is a sound management option that could prevent detrimental effects in patients awaiting kidney transplantation.
Figures
References
-
- Sautner T, Gnant M, Banhegyi C, Wamser P, Gotzinger P, Steininger R, Muhlbacher F. Risk factors for development of panel reactive antibodies and their impact on kidney transplantation outcome. Transpl Int. 1992;14(SUPPL. 1):S116–S120. - PubMed
-
- Centers for Medicare & Medicaid Services. End-Stage Renal Disease Prospective Payment System. Regulation Number 1418-F. Available at http://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/ESRDpayment....
-
- Centers for Medicare & Medicaid Services. Final CY 2013 End-Stage Renal Disease Prospective Payment System. Regulation Number 1352-F. Available at http://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/ESRDpayment....
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
