

Nitroxyl (HNO): A novel approach for the acute treatment of heart failure
- PMID: 24107588
- PMCID: PMC4110196
- DOI: 10.1161/CIRCHEARTFAILURE.113.000632
Nitroxyl (HNO): A novel approach for the acute treatment of heart failure
Abstract
Background: The nitroxyl (HNO) donor, Angeli's salt, exerts positive inotropic, lusitropic, and vasodilator effects in vivo that are cAMP independent. Its clinical usefulness is limited by chemical instability and cogeneration of nitrite which itself has vascular effects. Here, we report on effects of a novel, stable, pure HNO donor (CXL-1020) in isolated myoctyes and intact hearts in experimental models and in patients with heart failure (HF).
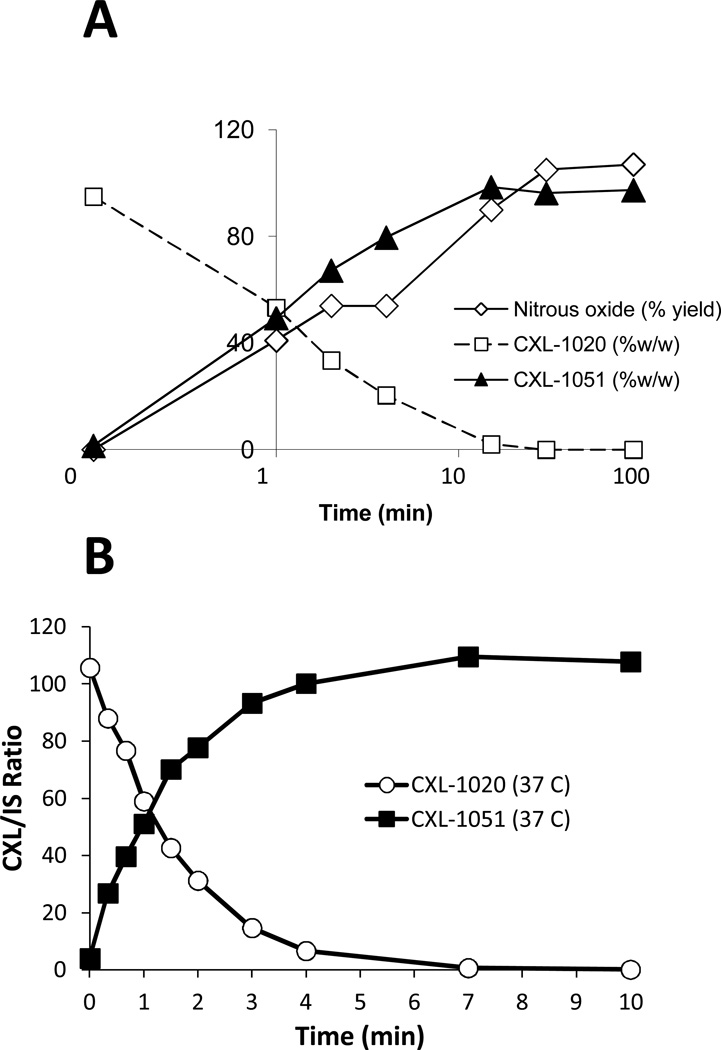
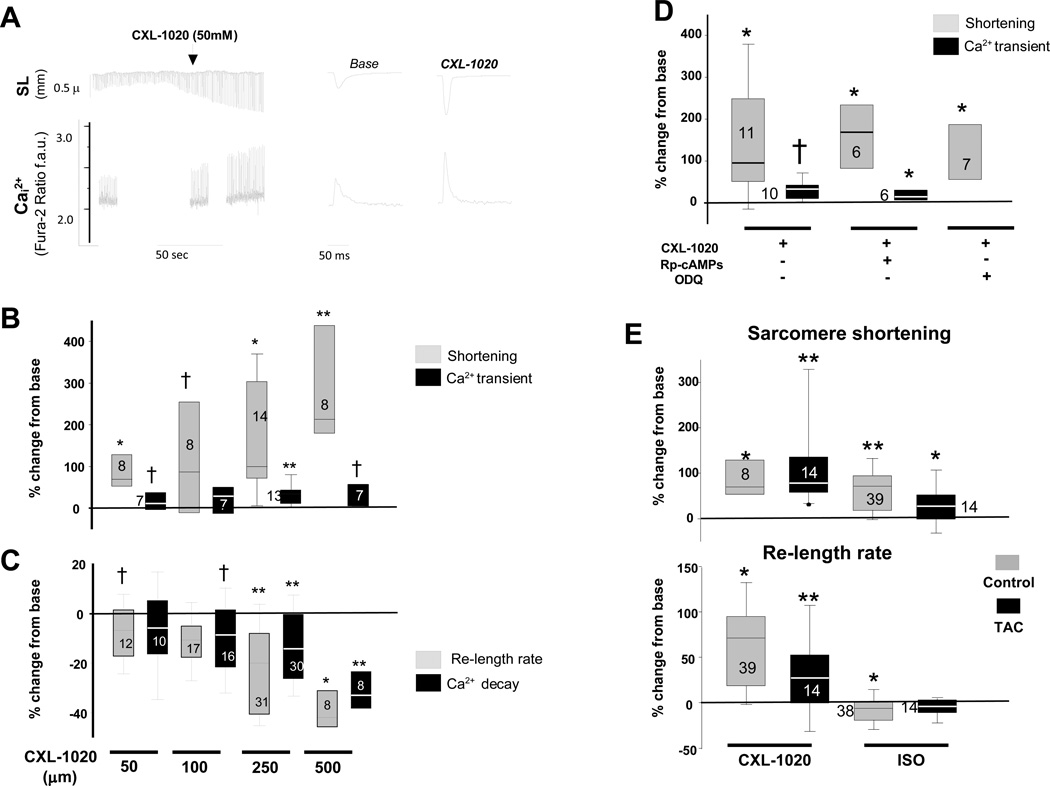
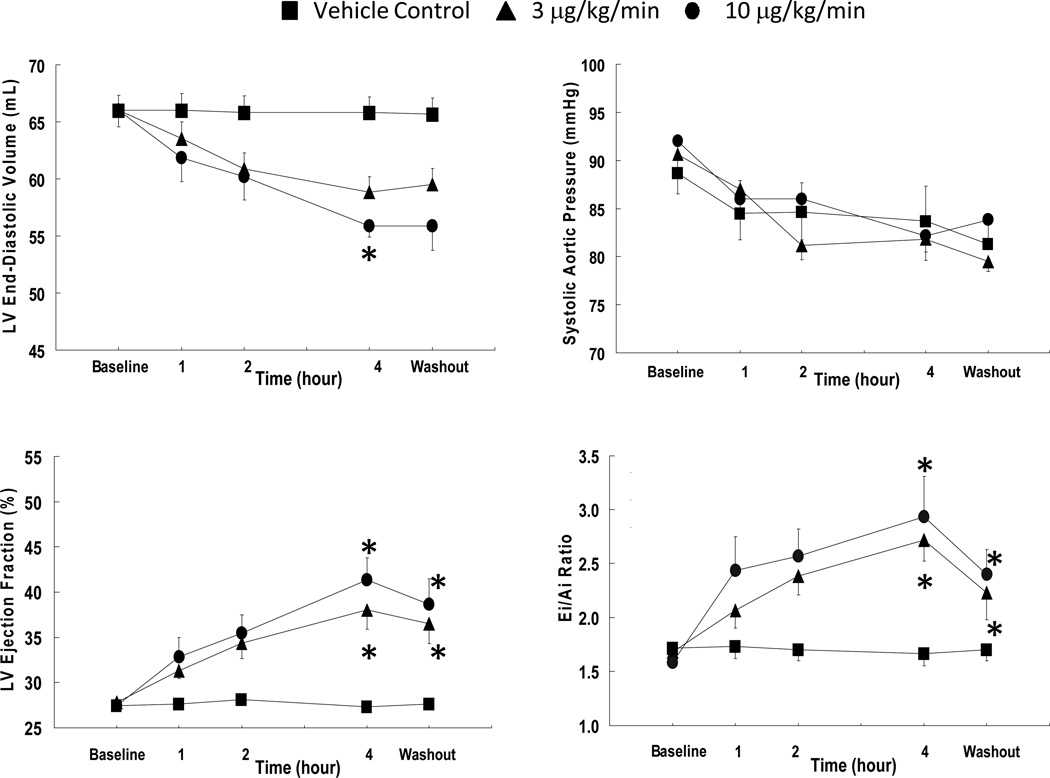
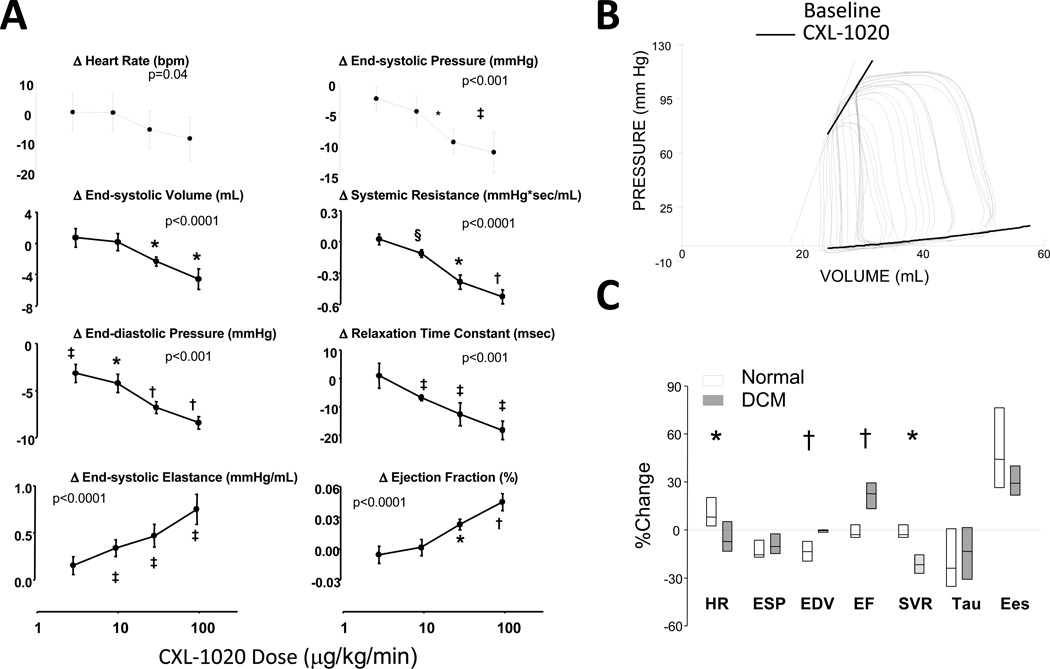
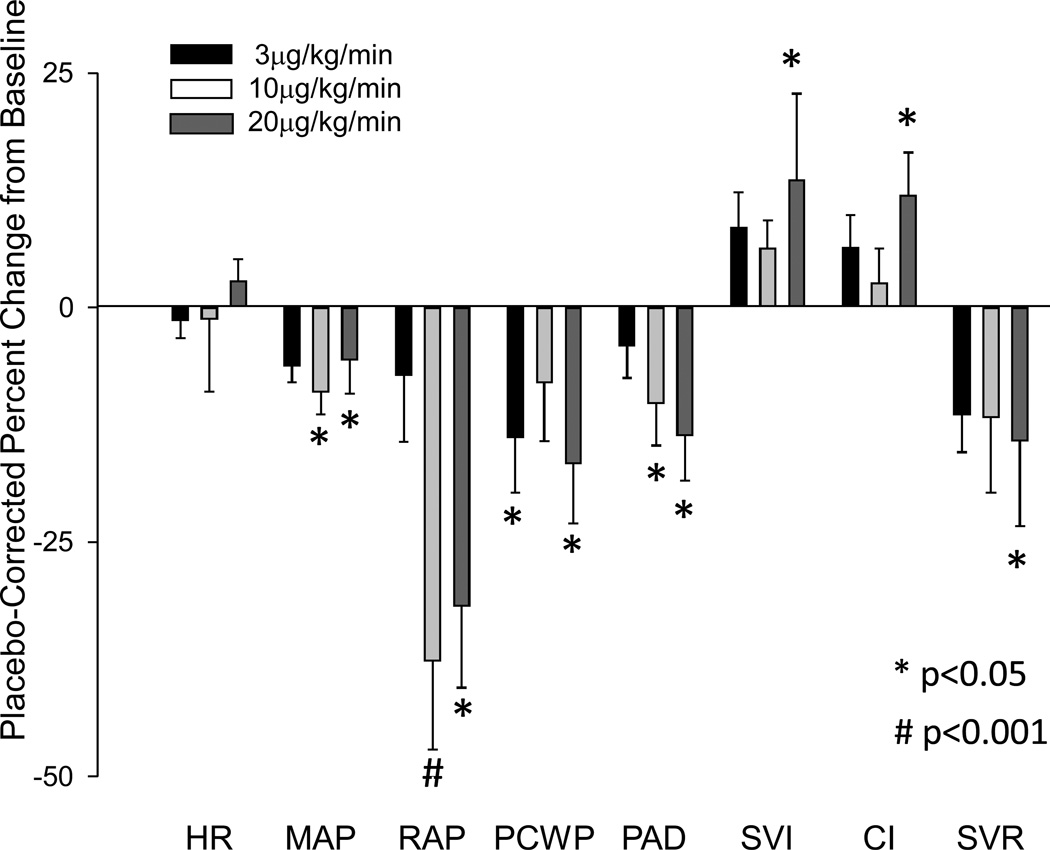
Methods and results: CXL-1020 converts solely to HNO and inactive CXL-1051 with a t1/2 of 2 minutes. In adult mouse ventricular myocytes, it dose dependently increased sarcomere shortening by 75% to 210% (50-500 μmol/L), with a ≈30% rise in the peak Ca(2+) transient only at higher doses. Neither inhibition of protein kinase A nor soluble guanylate cyclase altered this contractile response. Unlike isoproterenol, CXL-1020 was equally effective in myocytes from normal or failing hearts. In anesthetized dogs with coronary microembolization-induced HF, CXL-1020 reduced left ventricular end-diastolic pressure and myocardial oxygen consumption while increasing ejection fraction from 27% to 40% and maximal ventricular power index by 42% (both P<0.05). In conscious dogs with tachypacing-induced HF, CXL-1020 increased contractility assessed by end-systolic elastance and provided venoarterial dilation. Heart rate was minimally altered. In patients with systolic HF, CXL-1020 reduced both left and right heart filling pressures and systemic vascular resistance, while increasing cardiac and stroke volume index. Heart rate was unchanged, and arterial pressure declined modestly.
Conclusions: These data show the functional efficacy of a novel pure HNO donor to enhance myocardial function and present first-in-man evidence for its potential usefulness in HF.
Clinical trial registration: URL: http://www.clinicaltrials.gov. Unique identifiers: NCT01096043, NCT01092325.
Keywords: cardiomyopathies; heart contractility; humans; muscle cells; nitroxyl; pharmacology; vasodilator drugs.
Figures
References
-
- Abraham WT, Fonarow GC, Albert NM, Stough WG, Gheorghiade M, Greenberg BH, O'Connor CM, Sun JL, Yancy CW, Young JB. Predictors of in-hospital mortality in patients hospitalized for heart failure: Insights from the organized program to initiate lifesaving treatment in hospitalized patients with heart failure (optimize-hf) J Am Coll Cardiol. 2008;52:347–356. - PubMed
-
- Oliva F, Mortara A, Cacciatore G, Chinaglia A, Di Lenarda A, Gorini M, Metra M, Senni M, Maggioni AP, Tavazzi L. Acute heart failure patient profiles, management and in-hospital outcome: Results of the italian registry on heart failure outcome. Eur J Heart Fail. 2012;14:1208–1217. - PubMed
-
- Greenberg B. Acute decompensated heart failure - treatments and challenges. Circulation Journal. 2012;76:532–543. - PubMed
-
- Felker GM, Mentz RJ. Diuretics and ultrafiltration in acute decompensated heart failure. J Am Coll Cardiol. 2012;59:2145–2153. - PubMed
-
- Majure DT, Teerlink JR. Update on the management of acute decompensated heart failure. Current Treatment Options in Cardiovascular Medicine. 2011;13:570–585. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
