

Potential use of biomarkers in acute kidney injury: report and summary of recommendations from the 10th Acute Dialysis Quality Initiative consensus conference
- PMID: 24107851
- PMCID: PMC4198530
- DOI: 10.1038/ki.2013.374
Potential use of biomarkers in acute kidney injury: report and summary of recommendations from the 10th Acute Dialysis Quality Initiative consensus conference
Abstract
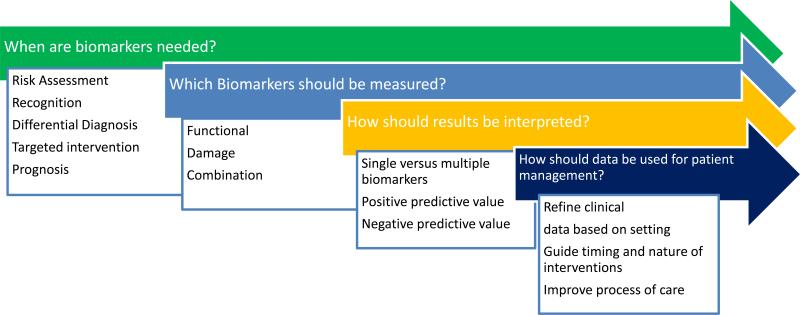
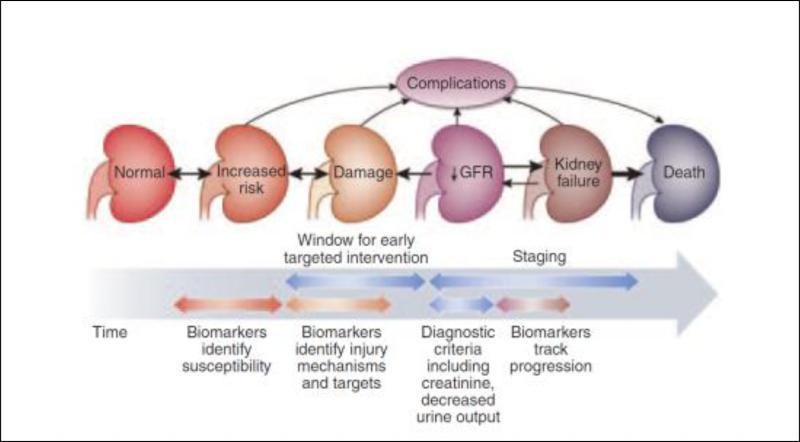
Over the last decade there has been considerable progress in the discovery and development of biomarkers of kidney disease, and several have now been evaluated in different clinical settings. Although there is a growing literature on the performance of various biomarkers in clinical studies, there is limited information on how these biomarkers would be utilized by clinicians to manage patients with acute kidney injury (AKI). Recognizing this gap in knowledge, we convened the 10th Acute Dialysis Quality Initiative meeting to review the literature on biomarkers in AKI and their application in clinical practice. We asked an international group of experts to assess four broad areas for biomarker utilization for AKI: risk assessment, diagnosis, and staging; differential diagnosis; prognosis and management; and novel physiological techniques including imaging. This article provides a summary of the key findings and recommendations of the group, to equip clinicians to effectively use biomarkers in AKI.
Figures
References
-
- Singbartl K, Kellum JA. AKI in the ICU: definition, epidemiology, risk stratification, and outcomes. Kidney Int. 2011 - PubMed
-
- Stewart J FG, Smith N, Kelly K, Mason M. Adding insult to injury: a review of the care of patients who died in hospital with a primary diagnosis of acute kidney injury (acute renal failure). A report by the National Confidential Enquiry into Patient Outcome and Death. 2009 http://www ncepodorguk/2009akihtm 2009.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
