

Influence of patient, physician, and hospital factors on 30-day readmission following pancreatoduodenectomy in the United States
- PMID: 24108580
- PMCID: PMC3983984
- DOI: 10.1001/jamasurg.2013.2509
Influence of patient, physician, and hospital factors on 30-day readmission following pancreatoduodenectomy in the United States
Abstract
IMPORTANCE It is not known whether hospital and surgeon volumes have an association with readmission among patients undergoing pancreatoduodenectomy.
Objective: To evaluate patient-, surgeon-, and hospital-level factors associated with readmission.
Design, setting, and participants: Retrospective cohort study using the Surveillance, Epidemiology, and End Results (SEER)-Medicare data with cases diagnosed from January 1, 1998, to December 31, 2005, and followed up until December 2007. Population-based cancer registry data were linked to Medicare data for the corresponding patients. A total of 1488 unique individuals who underwent a pancreatoduodenectomy were identified.
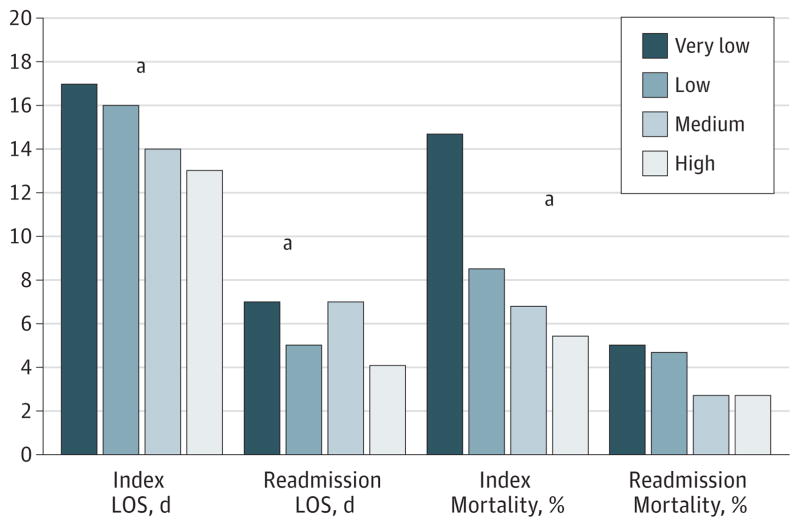
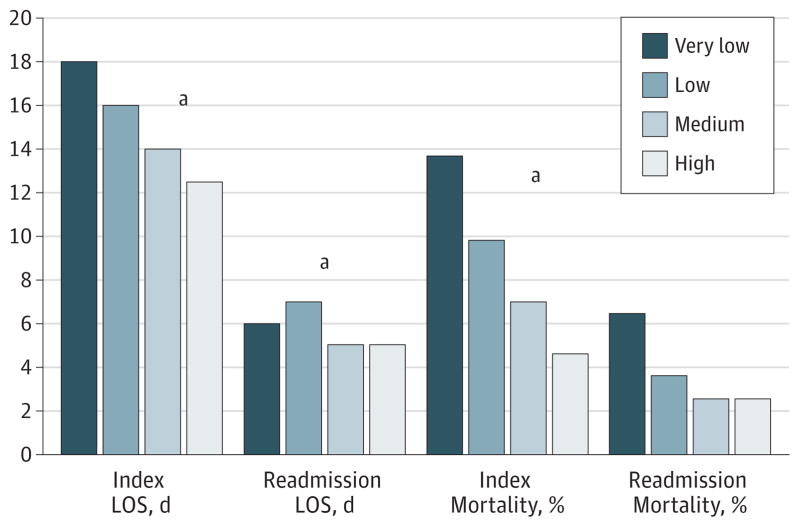
Interventions: Undergoing pancreatoduodenectomy at hospitals classified by volume of pancreatoduodenectomy procedures performed at the facility were either very-low, low, medium, or high volume. Undergoing pancreatoduodenectomy by surgeons classified by volume of pancreatoduodenectomy procedures performed by the surgeon were either very-low, low, medium, or high volume.
Main outcomes and measures: In-hospital morbidity, mortality, and 30-day readmission were examined.
Results: The median age was 74 years, and 1436 patients (96.5%) had a least 1 medical comorbidity. Patients were treated by 575 distinct surgeons at 298 distinct hospitals. Length of stay was longest (median, 17 days) and 90-day mortality highest (17.2%) at very-low-volume hospitals (P < .001). Among all pancreatoduodenectomy patients, 292 (21.3%) were readmitted within 30 days of discharge. There was no effect of surgeon volume and a modest effect of hospital volume (odds ratio for highest- vs lowest-volume quartiles, 1.85; 95% CI, 1.22-2.80; P = .02). The presence of significant preoperative medical comorbidities was associated with an increased risk for hospital readmission after pancreatoduodenectomy. A comorbidity score greater than 13 had a pronounced effect on the chance of readmission following pancreatoduodenectomy (odds ratio, 2.06; 95% CI, 1.56-2.71; P < .001). The source of variation in readmission was primarily attributable to patient-related factors (95.4%), while hospital factors accounted for 4.3% of the variability and physician factors for only 0.3%.
Conclusions and relevance: Nearly 1 in 5 patients are readmitted following pancreatoduodenectomy. While variation in readmission is, in part, attributable to differences among hospitals, the largest share of variation was found at the patient level.
Conflict of interest statement
Figures
Comment in
-
Readmissions following pancreatoduodenectomy: it's when things don't go well that experienced pancreatic surgeons earn their keep.JAMA Surg. 2013 Dec;148(12):1102. doi: 10.1001/jamasurg.2013.2528. JAMA Surg. 2013. PMID: 24108544 No abstract available.
References
-
- Jencks SF. Defragmenting care. Ann Intern Med. 2010;153(11):757–758. - PubMed
-
- Hansen LO, Young RS, Hinami K, Leung A, Williams MV. Interventions to reduce 30-day rehospitalization: a systematic review. Ann Intern Med. 2011;155(8):520–528. - PubMed
-
- Martin RC, Brown R, Puffer L, et al. Readmission rates after abdominal surgery: the role of surgeon, primary caregiver, home health, and subacute rehab. Ann Surg. 2011;254(4):591–597. - PubMed
-
- Yermilov I, Bentrem D, Sekeris E, et al. Readmissions following pancreaticoduodenectomy for pancreas cancer: a population-based appraisal. Ann Surg Oncol. 2009;16(3):554–561. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
