

Obstructive sleep apnea in children: a critical update
- PMID: 24109201
- PMCID: PMC3792928
- DOI: 10.2147/NSS.S51907
Obstructive sleep apnea in children: a critical update
Abstract
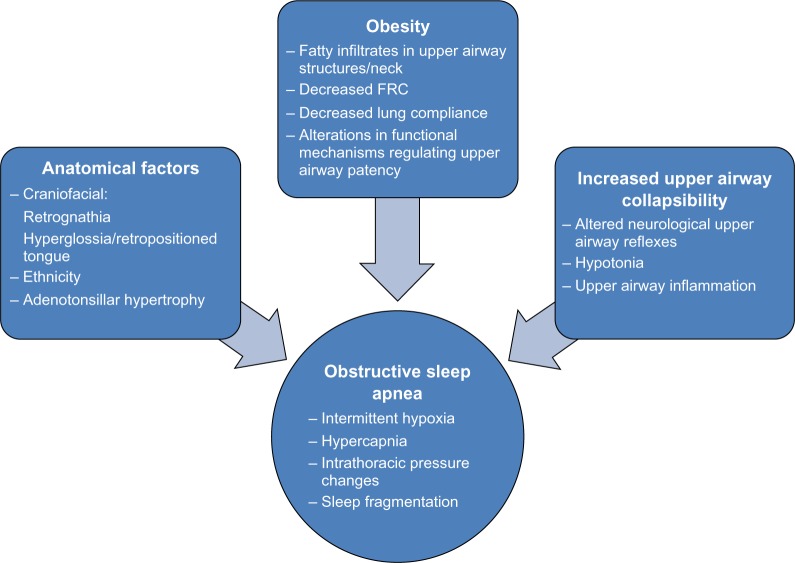
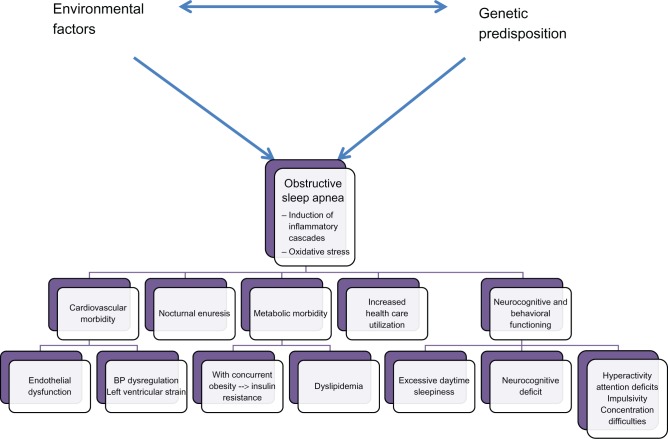
Obstructive sleep apnea (OSA) in children is a highly prevalent disorder caused by a conglomeration of complex pathophysiological processes, leading to recurrent upper airway dysfunction during sleep. The clinical relevance of OSA resides in its association with significant morbidities that affect the cardiovascular, neurocognitive, and metabolic systems. The American Academy of Pediatrics recently reiterated its recommendations that children with symptoms and signs suggestive of OSA should be investigated with polysomnography (PSG), and treated accordingly. However, treatment decisions should not only be guided by PSG results, but should also integrate the magnitude of symptoms and the presence or absence of risk factors and signs of OSA morbidity. The first-line therapy in children with adenotonsillar hypertrophy is adenotonsillectomy, although there is increasing evidence that medical therapy, in the form of intranasal steroids or montelukast, may be considered in mild OSA. In this review, we delineate the major concepts regarding the pathophysiology of OSA, its morbidity, diagnosis, and treatment.
Keywords: adenotonsillar hypertrophy; morbidity; pathophysiology; pediatric sleep disordered breathing; polysomnography; treatment.
Figures
References
-
- Kheirandish-Gozal L, Gozal D, editors. Sleep Disordered Breathing in Children A Comprehensive Clinical Guide to Evaluation and Treatment. New York, NY: Springer Science; 2012.
-
- Li AM, So HK, Au CT, et al. Epidemiology of obstructive sleep apnoea syndrome in Chinese children: a two-phase community study. Thorax. 2010;65(11):991–997. - PubMed
-
- Marcus CL, Brooks LJ, Draper KA, et al. American Academy of Pediatrics Diagnosis and management of childhood obstructive sleep apnea syndrome. Pediatrics. 2012;130(3):e714–e755. - PubMed
-
- Rosen CL, Larkin EK, Kirchner HL, et al. Prevalence and risk factors for sleep-disordered breathing in 8- to 11-year-old children: association with race and prematurity. J Pediatr. 2003;142(4):383–389. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
