

Geometry of the randomized evidence for treatments of pulmonary hypertension
- PMID: 24112824
- PMCID: PMC4480770
- DOI: 10.1111/1755-5922.12050
Geometry of the randomized evidence for treatments of pulmonary hypertension
Abstract
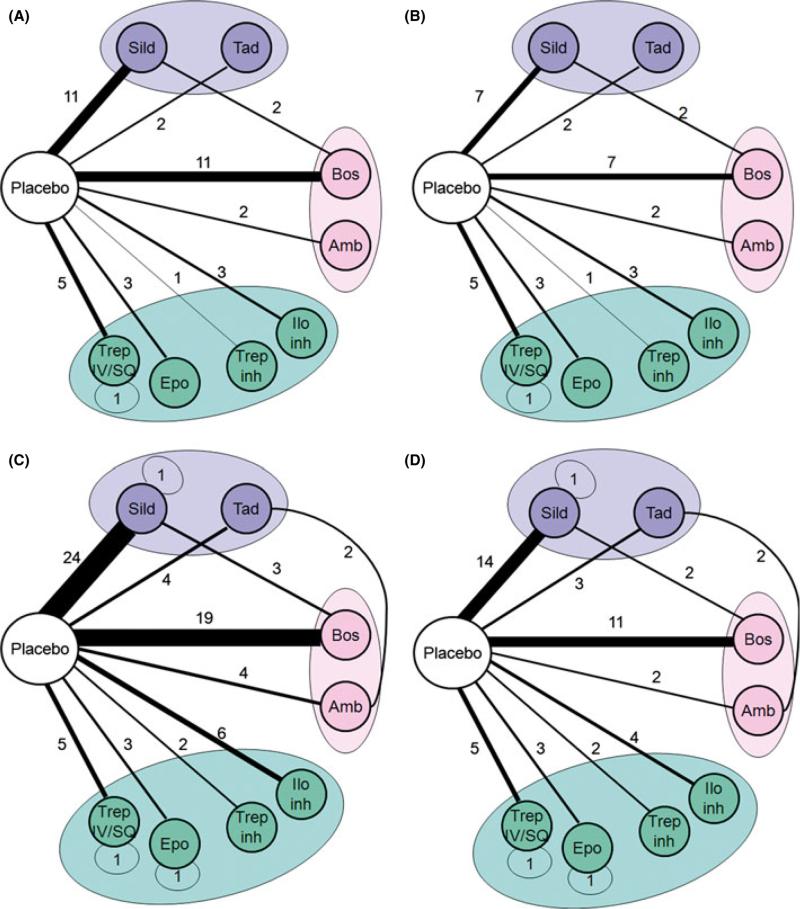
Objective: We studied the entire agenda of randomized clinical trials in pulmonary hypertension (PH) using sociological methods. We explored the geometry of the PH network to interpret the evidence on multiple competing treatments for the same indication.
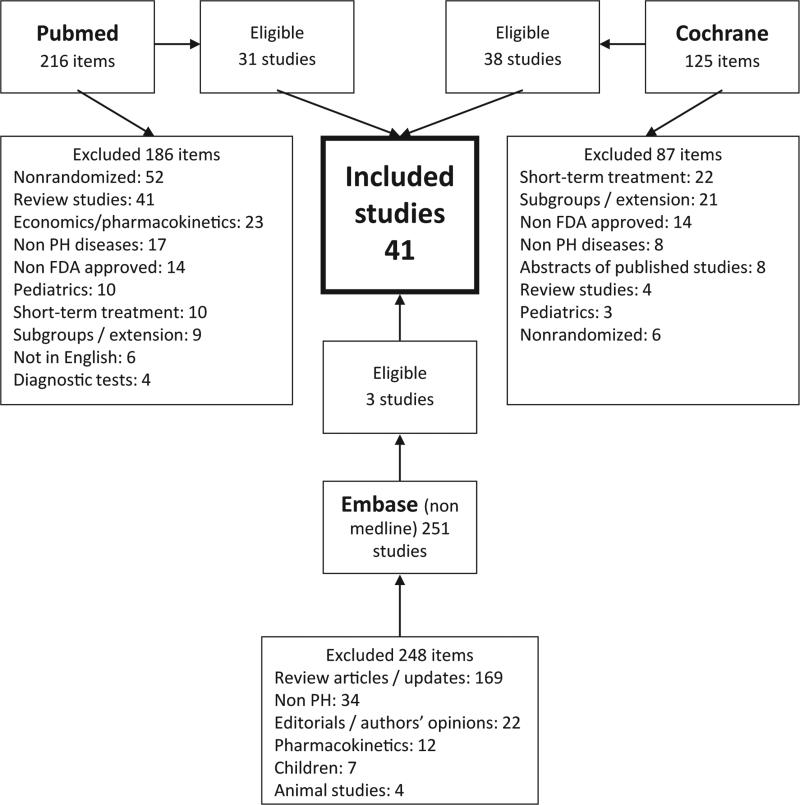
Design: We searched MEDLINE, Embase and Cochrane Library Databases for published studies. We queried clinicaltrials.gov and WHO International Clinical Trials Registry platform for non-published studies.
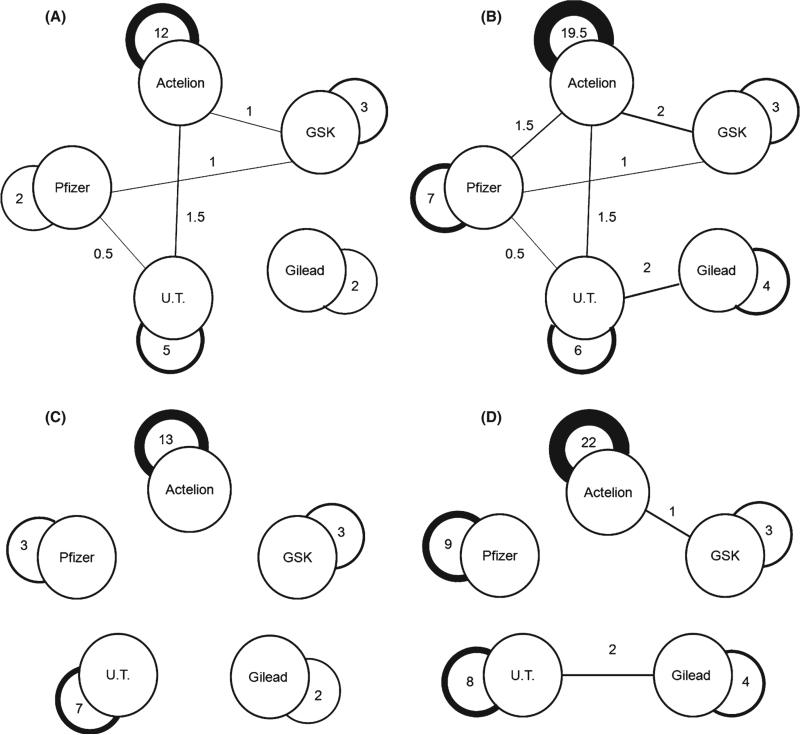
Results: We found 75 randomized trials (41 published [n = 4136 participants] and 34 registered unpublished [planned n = 3470 participants]). Of the published randomized studies, all used placebo as the comparator arm except for two nonindustry-sponsored comparisons between phosphodiestearase-5 (PDE-5) inhibitors and endothelin receptor antagonists (ERA), and one study comparing two different regimens of treprostinil. Similarly, only five unpublished/ongoing trials used an active PH treatment as comparator (PDE-5 inhibitors versus ERA (n = 3), different doses of sildenafil (n = 1) and two formulations of epoprostenol (n = 1). Of the 75 trials, 47 were sponsored by the manufacturer of the tested active product(s), and only two trials were sponsored by two companies comparing their products.
Conclusions: The relative merits of different treatment options are not directly known, as there are very few head-to-head comparisons. A limited number of ongoing studies are using active FDA-approved PH-treatments for comparison. This lack of information can be overcome by carefully designing comparative effectiveness trials.
Keywords: Pulmonary hypertension; Treatment.
© 2013 John Wiley & Sons Ltd.
Figures
References
-
- McLaughlin VV, Archer SL, Badesch DB, et al. ACCF/AHA 2009 expert consensus document on pulmonary hypertension: a report of the American College of Cardiology Foundation Task Force on Expert Consensus Documents and the American Heart Association: developed in collaboration with the American College of Chest Physicians, American Thoracic Society, Inc., and the Pulmonary Hypertension Association. Circulation. 2009;119:2250–2294. - PubMed
-
- Simonneau G, Robbins IM, Beghetti M, et al. Updated clinical classification of pulmonary hypertension. J Am Coll Cardiol. 2009 Jun 30;54(1 Suppl.):S43–S54. - PubMed
-
- Salanti G, Higgins JP, Ades AE, Ioannidis JP. Evaluation of networks of randomized trials. Stat Methods Med Res. Jun. 2008;17:279–301. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
