

Review
doi: 10.1161/JAHA.113.000338.
The advancing field of cell-based therapy: insights and lessons from clinical trials
Affiliations
- PMID: 24113326
- PMCID: PMC3835242
- DOI: 10.1161/JAHA.113.000338
Item in Clipboard
Review
The advancing field of cell-based therapy: insights and lessons from clinical trials
J Am Heart Assoc.
.
No abstract available
Keywords: cardiomyopathy; cardiovascular interventional therapy; stem cells.
Figures
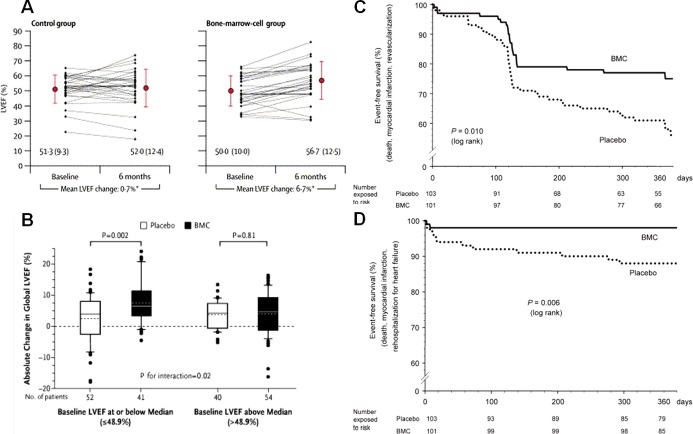
Benefits of bone marrow mononuclear cell (BM‐MNC) therapy. A and B, Intracoronary BM‐MNC delivery led to a 6.7% point improvement in left ventricular ejection fraction (LVEF) at 6 months in the BOOST clinical trial and to 5.5% improvement in LVEF at 4 months in the REPAIR‐AMI clinical trial, respectively. C, Kaplan–Meier event‐free survival analysis in the REPAIR‐AMI at 12 months showed better survival from death, recurrence of myocardial infarction, or revascularization procedures and (D) death, recurrence of myocardial infarction, or rehospitalization for heart failure in the BM‐MNC group. Panel A was reproduced with permission from Wollert et al, Lancet, 2004, panel B from Schachinger et al, New England Journal of Medicine, 2006, and panels C and D from Schachinger et al, European Heart Journal, 2006. BOOST indicates BOne marrOw transfer to enhance ST‐elevation infarct regeneration; REPAIR‐AMI, Reinfusion of Enriched Progenitor Cells and Infarct Remodeling in Acute Myocardial Infarction.
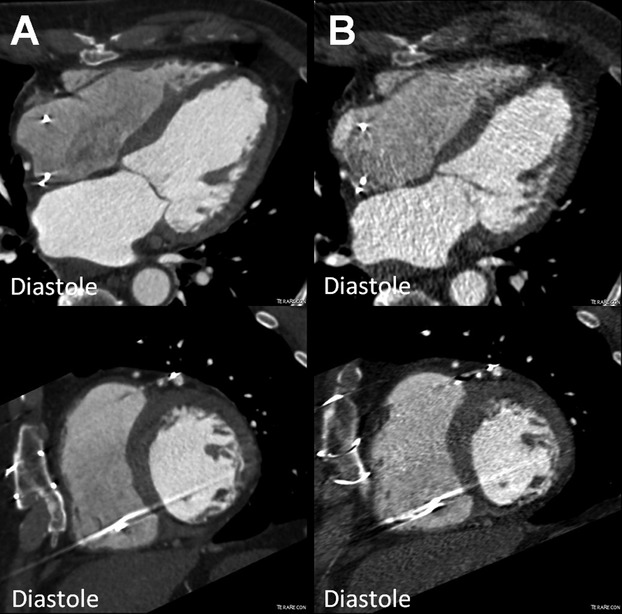
Reduction of left ventricular end‐diastolic volume (EDV) in the POSEIDON study. MDCT images (4 chamber and short axis view) of a patient with chronic ischemic cardiomyopathy (A) before (EDV 176.1 mL) and (B) after transendocardial stem cell injection (TESI) with 20 million autologous mesenchymal stem cells (EDV 136.8 mL). MDCT indicates multi‐detector computer tomography; POSEIDON, PercutaneOus StEm Cell Injection Delivery Effects On Neomyogenesis.
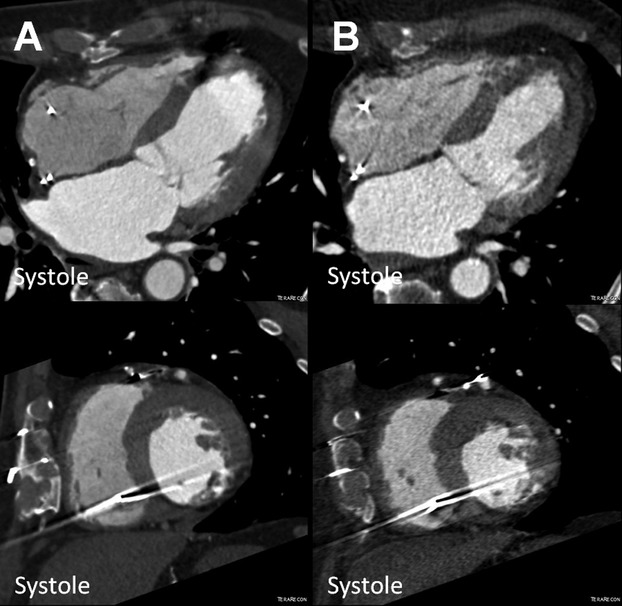
Reduction of left ventricular end‐systolic volume (ESV) in the POSEIDON study. MDCT images (4 chamber and short axis view) of a patient with chronic ischemic cardiomyopathy (A) before (ESV 126.9 mL) and (B) after transendocardial stem cell injection (TESI) with 20 million autologous MSCs (ESV 77.1 mL). MDCT indicates multi‐detector computer tomography; MSCs, mesenchymal stem cells; POSEIDON, PercutaneOus StEm Cell Injection Delivery Effects On Neomyogenesis.
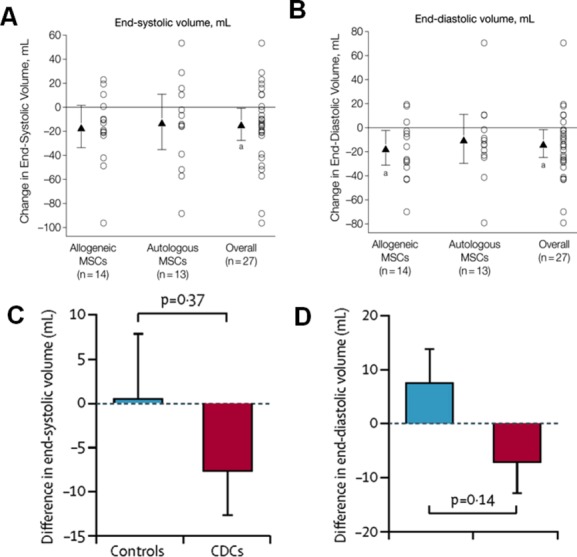
Comparison of end‐systolic and end‐diastolic volumes in POSEIDON and CADUCEUS trials. A and B, Chamber volumes in POSEIDON trial. Mean changes from baseline to 13 months are noted by triangles and depict changes in cardiac phenotype assessed by cardiac MDCT scan. Error bars indicate 95% CIs. Individual patient changes from baseline are shown as circles. Shown are changes in cardiac volumes from baseline to 13‐month follow‐up in allogeneic, autologous, and overall patient groups. Within‐group P values are noted as a P<0.05. C and D, Chamber volumes in CADUCEUS study participants. C, Treatment effects (baseline vs 6 months) for end‐systolic volume. D, Treatment effects (baseline vs 6 months) for end‐diastolic volume. Panels A and B are reproduced with permission from Hare et al, JAMA, 2012. Panels C and D are reproduced with permission from Makkar et al, Lancet, 2012. CADUCEUS indicates Cardiosphere‐Derived aUtologous stem Cells to reverse ventricUlar dySfunction; CDCs, cardiosphere‐derived cells; CIs, confidence intervals; MDCT, multi‐detector computer tomography; MSCs, mesenchymal stem cells; POSEIDON, PercutaneOus StEm Cell Injection Delivery Effects On Neomyogenesis.
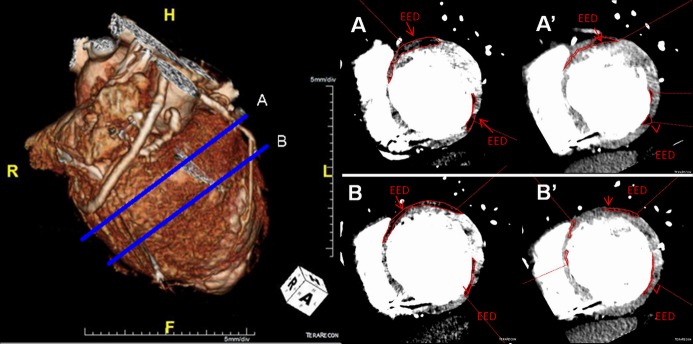
Reduction of scar size (POSEIDON clinical trial). (Left) MDCT 3D reconstruction image with (Right) respective (A) basal and (B) midventricular short axis images of a patient with chronic ischemic cardiomyopathy with a scar size (MDCT‐EED outlined in red) of (A and B) 40.34 g and its reduction to (A' and B') 26.35 g after transendocardial stem cell injection (TESI) with allogeneic MSCs (100 million). EED indicates early enhancement defect; MDCT, multi‐detector computer tomography; MSCs, mesenchymal stem cells; POSEIDON, PercutaneOus StEm Cell Injection Delivery Effects On Neomyogenesis.
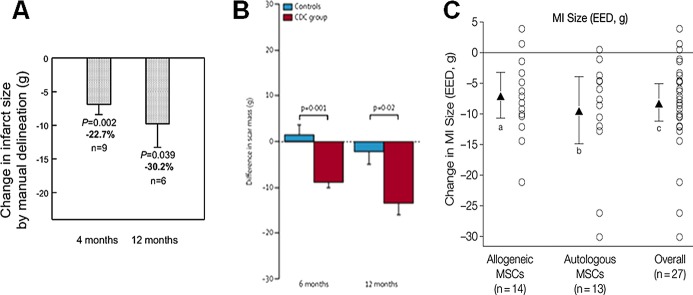
Comparison of scar size reduction in (A) SCIPIO, (B) CADUCEUS, and (C) POSEIDON trials. A, SCIPIO Trial 1‐year follow‐up shows infarct size reduction at 4 and 12 months after CSC therapy. B, CADUCEUS trial showed decreases in scar mass and increases in viable mass on MRI in patients treated with CDCs but not controls. C, Myocardial infarct (MI) size reduction shown in POSEIDON trial. Panel A reproduced with permission from Chugh et al, Circulation, 2012; panel B from Makkar et al, Lancet, 2012; and panel C from Hare et al, JAMA, 2012. CADUCEUS indicates Cardiosphere‐Derived aUtologous stem Cells to reverse ventricUlar dySfunction; CDC, cardiosphere‐derived cell; CSCs, cardiac stem cells; EED, early enhancement defect; MRI, magnetic resonance imaging; MSCs, mesenchymal stem cells; POSEIDON, PercutaneOus StEm Cell Injection Delivery Effects On Neomyogenesis; SCIPIO, Stem Cell Infusion in Patients with Ischemic cardiomyopathy.
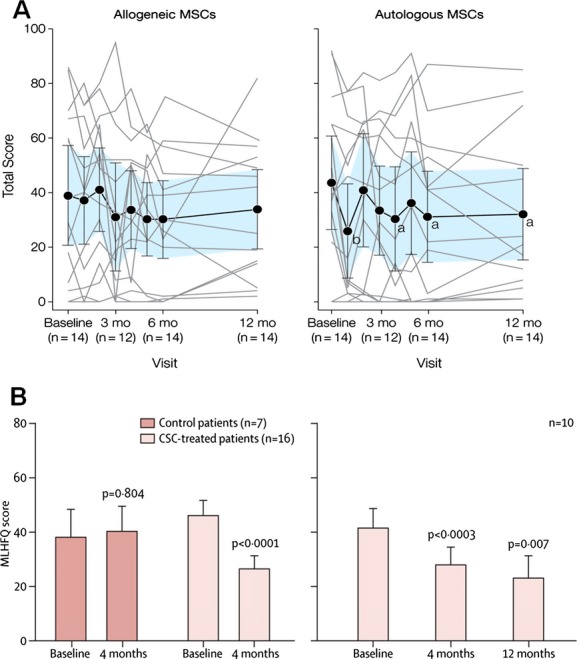
Comparison of MLHFQ scores in POSEIDON and SCIPIO trials. A, POSEIDON trial showed improvement in MLHFQ score in the autologous MSC group at the 6‐ and 12‐month time points. B, SCIPIO trial demonstrated continuous improvement in MLHFQ score at 4 and 12 months. Panel A reproduced with permission from Hare et al, JAMA, 2012 and panel B from Chugh et al, Circulation, 2012. CSCs indicates cardiac stem cells; MLHFQ, Minnesota Living with Heart Failure Questionnaire; MSC, mesenchymal stem cell; POSEIDON, PercutaneOus StEm Cell Injection Delivery Effects On Neomyogenesis; SCIPIO, Stem Cell Infusion in Patients with Ischemic cardiomyopathy.
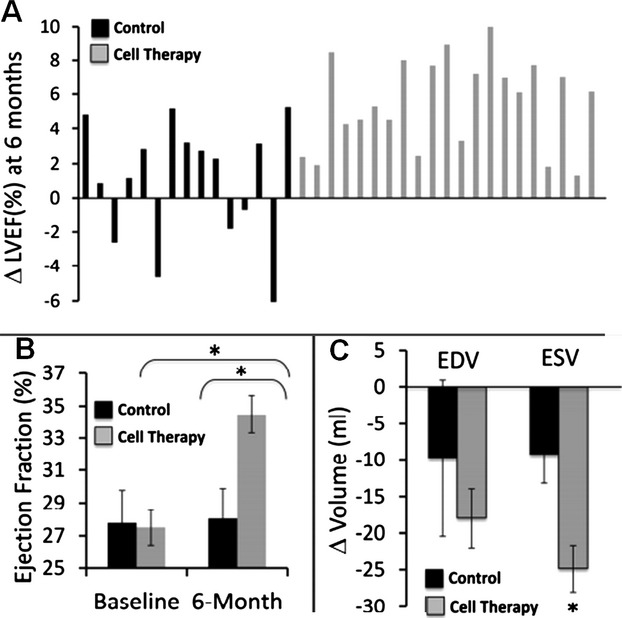
Greater reversal of remodeling after autologous cardiopoietic stem cell therapy at 6‐month follow‐up (C‐CURE trial). A, Changes in left ventricular ejection fraction (LVEF) for each individual patient. Control group (black) includes patients that received standard of care alone. Cell therapy group (gray) includes patients that received standard of care plus cardiopoietic stem cells. B, Median values for LVEF prior to and 6‐months following treatment. C, Changes in left ventricular end‐diastolic (ED) and end‐systolic (ES) volumes. Reproduced with permission from Bartunek et al, JACC, 2013.
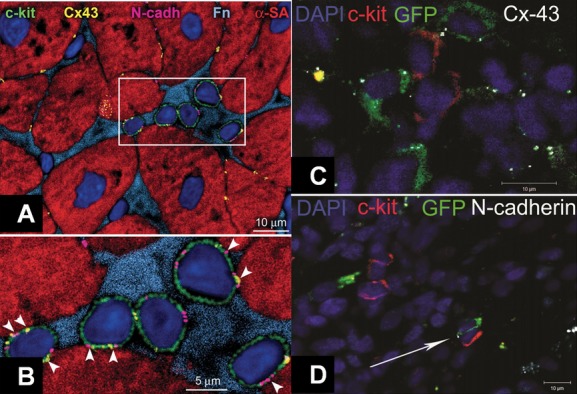
Human cardiac stem cell (CSC) niche in the myocardium. A, c‐kit+ (green) human cardiac stem cells (hCSCs) are nested in the interstitium and are surrounded by fibronectin (Fn, bright blue). These hCSCs are connected by gap junctions represented by connexin 43 (Cx43, yellow dots) and adherens junctions shown by N‐cadherin (N‐cadh, magenta) to cardiomyocytes (α‐sarcomeric actin, α‐SA, red). B, These cell‐to‐cell communications between CSCs and cardiomyocytes are indicated by arrowheads. C, Cell–Cell interactions between endogenous and exogenous stem cells. C and D, Immature mesenchymal stem cells (MSCs, green) are found within the swine myocardium to interact with resident c‐kit+ CSCs (red) by connexin‐43 (C, white) and N‐cadherin (D, white arrow) connections, closely resembling CSC niches. Panels A and B reproduced with permission from Leri et al, Circulation, 2013, panels C and D from Hatzistergos et al, Circulation Research 2010.DAPI indicates 4',6‐diamidino‐2‐phenylindole; GFP, green fluorescent protein.
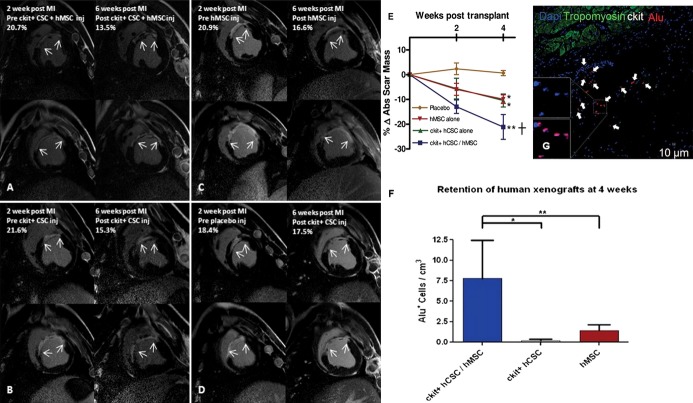
Human c‐kit+ cardiac stem cells (CSCs) and bone marrow mesenchymal stem cells (MSCs) reduce infarct size and enhance engraftment in a porcine model. A through D, Delayed enhancement CMR images showing pre‐injection scar and 4‐weeks post‐injection scar changes (white arrows indicate infarct extension). E, Reduction in absolute infarct size from preinjection to 4 weeks post‐injection (*P<0.05 within group ANOVA; †P<0.05 vs placebo at 4 weeks post‐injection by Bonferroni posttest). F, Immunohistochemical‐stained images showing clusters of Alu‐positive human stem cells (white arrows) engrafted in the infarct territory. G, Retention of Alu+ human stem cells was 7‐fold higher when hCSCs and hMSCs were injected together compared with either cell type administered alone (n=3 analyzed per treatment group). Graphs represent mean±SEM *P<0.001 and **P<0.05, between‐group 1‐way ANOVA. Reproduced with permission from Williams et al, Circulation, 2013. ANOVA indicates analysis of variance; CMR, cardiovascular magnetic resonance; MI, myocardial infarction; SEM, standard error of the mean.
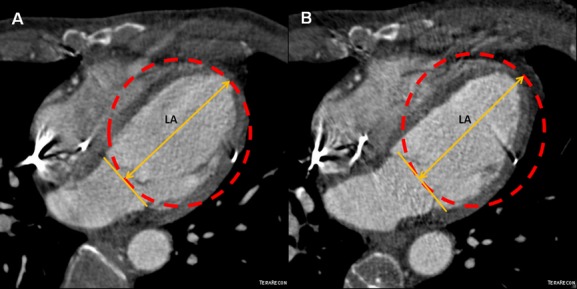
Reversal of remodeling as reduction of sphericity index in the POSEIDON trial. A, Four chamber MDCT images of a chronic ischemic cardiomyopathy patient with a sphericity index of 0.48 and (B) its reduction to 0.41 after transendocardial stem cell injection (TESI) with allogeneic mesenchymal stem cells (MSCs, 20 million). Sphericity index was calculated as: EDV/volume of sphere using long axis (LA) as diameter. EDV indicates end‐diastolic volume; MDCT, multi‐detector computer tomography; POSEIDON, PercutaneOus StEm Cell Injection Delivery Effects On Neomyogenesis.
References
-
- Hare JM, Fishman JE, Gerstenblith G, Difede Velazquez DL, Zambrano JP, Suncion VY, Tracy M, Ghersin E, Johnston PV, Brinker JA, Breton E, Davis‐Sproul J, Byrnes J, George R, Lardo A, Schulman IH, Mendizabal AM, Lowery MH, Rouy D, Altman P, Wong Po Foo C, Ruiz P, Amador A, Da Silva J, McNiece IK, Heldman AW. Comparison of allogeneic vs autologous bone marrow‐derived mesenchymal stem cells delivered by transendocardial injection in patients with ischemic cardiomyopathy: the POSEIDON randomized trial. JAMA. 2012; 308:1-11 - PMC - PubMed
-
- Bolli R, Chugh AR, D'Amario D, Loughran JH, Stoddard MF, Ikram S, Beache GM, Wagner SG, Leri A, Hosoda T, Sanada F, Elmore JB, Goichberg P, Cappetta D, Solankhi NK, Fahsah I, Rokosh DG, Slaughter MS, Kajstura J, Anversa P. Cardiac stem cells in patients with ischaemic cardiomyopathy (SCIPIO): initial results of a randomised phase 1 trial. Lancet. 2011; 378:1847-1857 - PMC - PubMed
-
- Bolli R, Chugh AR, D'Amario D, Loughran JH, Stoddard MF, Ikram S, Wagner SG, Beache GM, Leri A, Hosoda T, Goihberg P, Fiorini C, Solankhi N, Fahsah I, Elmore JB, Rokosh DG, Slaughter MS, Kajstura J, Anversa P. Effect of cardiac stem cells in patients with ischemic cardiomyopathy: interim results of the SCIPIO trial up to 2 years after therapy. Circulation. 2012; 126:2776-2799
-
- Chugh AR, Beache GM, Loughran JH, Mewton N, Elmore JB, Kajstura J, Pappas P, Tatooles A, Stoddard MF, Lima JA, Slaughter MS, Anversa P, Bolli R. Administration of cardiac stem cells in patients with ischemic cardiomyopathy: the SCIPIO trial: surgical aspects and interim analysis of myocardial function and viability by magnetic resonance. Circulation. 2012; 126:S54-S64 - PMC - PubMed
-
- Makkar RR, Smith RR, Cheng K, Malliaras K, Thomson LE, Berman D, Czer LS, Marban L, Mendizabal A, Johnston PV, Russell SD, Schuleri KH, Lardo AC, Gerstenblith G, Marban E. Intracoronary cardiosphere‐derived cells for heart regeneration after myocardial infarction (CADUCEUS): a prospective, randomised phase 1 trial. Lancet. 2012; 379:895-904 - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
