

Disease progression by infecting HIV-1 subtype in a seroconverter cohort in sub-Saharan Africa
- PMID: 24113395
- PMCID: PMC3815107
- DOI: 10.1097/QAD.0000000000000012
Disease progression by infecting HIV-1 subtype in a seroconverter cohort in sub-Saharan Africa
Abstract
Objective: To describe immunologic, virologic, and clinical HIV disease progression by HIV-1 subtype among Africans with well documented estimated dates of HIV infection (EDIs).
Design: Prospective cohort.
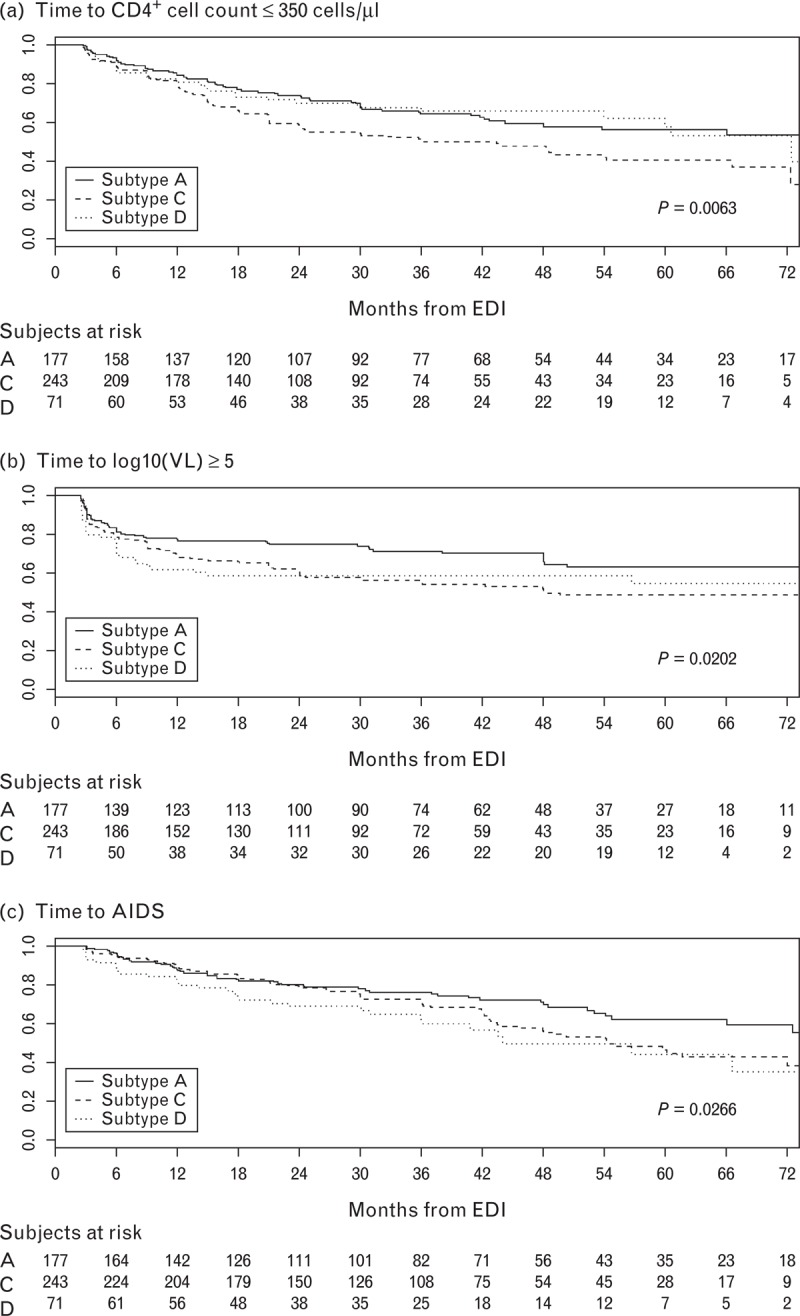
Methods: Adults and youth with documented HIV-1 infection in the past 12 months were recruited from seroincidence cohorts in East and Southern Africa and followed at 3-6 month intervals. Blood for lymphocyte subset and viral load determination was collected at each visit. Pol was sequenced from the first positive specimen to ascertain subtype. Preantiretroviral therapy disease progression was measured by three time-to-event endpoints: CD4 cell count 350 cells/μl or less, viral load measurement at least 1 × 10 copies/ml, and clinical AIDS.
Results: From 2006 to 2011, 615 participants were enrolled at nine research centers in Kenya, Rwanda, South Africa, Uganda, and Zambia; 579 (94.1%) had viral subtyping completed. Predominant subtypes were C (256, 44.2%), A (209, 36.1%), and D (84, 14.5%). After adjustment for age, sex, and human leukocyte antigen alleles in Cox regression analyses, subtype C-infected participants progressed faster than subtype A to all three endpoints [CD4 hazard ratio 1.60, 95% (confidence interval) CI 1.16, 2.20; viral load hazard ratio 1.59, 95% CI 1.12, 2.25; and AIDS hazard ratio 1.60, 95% CI 1.11, 2.31). Subtype D-infected participants reached high viral load more rapidly (hazard ratio 1.61, 95% CI 1.01, 2.57) and progressed nearly twice as fast to AIDS compared to subtype A (hazard ratio 1.93, 95% CI 1.21, 3.09).
Conclusion: Subtype-specific differences in HIV disease progression suggest that the local subtype distribution be considered when planning HIV programs and designing and defining clinical endpoints for HIV prevention trials.
Figures
References
-
- Laga M, Piot P. Prevention of sexual transmission of HIV: real results, science progressing, societies remaining behind. AIDS 2012; 26:1223–1229 - PubMed
-
- Hemelaar J, Gouws E, Ghys PD, Osmanov S. Global and regional distribution of HIV-1 genetic subtypes and recombinants in 2004. AIDS 2006; 20:W13–23 - PubMed
-
- Population Reference Bureau World Population Data Sheet, 2012: Washington, DC: Population Reference Bureau; 2012
-
- UNAIDS Global AIDS epidemic facts and figures, 2012: Geneva, Switzerland; UNAIDS; 2012
-
- Hessol NA, Koblin BA, van Griensven GJ, Bacchetti P, Liu JY, Stevens CE, et al. Progression of human immunodeficiency virus type 1 (HIV-1) infection among homosexual men in hepatitis B vaccine trial cohorts in Amsterdam, New York City, and San Francisco, 1978–1991. Am J Epidemiol 1994; 139:1077–1087 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
