

Database queries for hospitalizations for acute congestive heart failure: flexible methods and validation based on set theory
- PMID: 24113802
- PMCID: PMC3932461
- DOI: 10.1136/amiajnl-2013-001942
Database queries for hospitalizations for acute congestive heart failure: flexible methods and validation based on set theory
Abstract
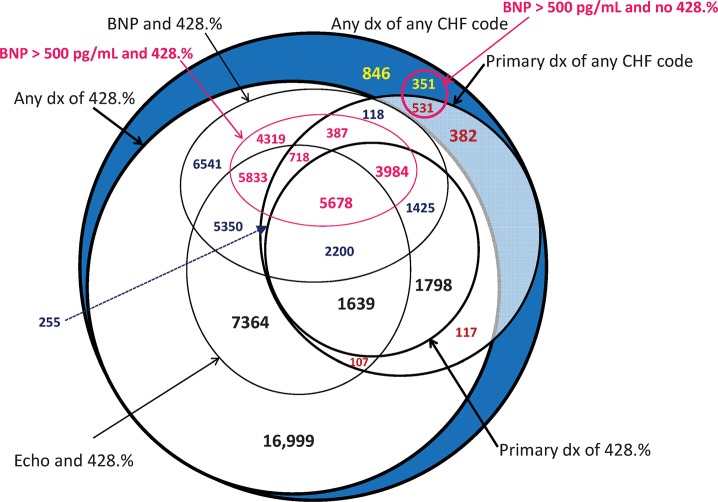
Background and objective: Electronic health records databases are increasingly used for identifying cohort populations, covariates, or outcomes, but discerning such clinical 'phenotypes' accurately is an ongoing challenge. We developed a flexible method using overlapping (Venn diagram) queries. Here we describe this approach to find patients hospitalized with acute congestive heart failure (CHF), a sampling strategy for one-by-one 'gold standard' chart review, and calculation of positive predictive value (PPV) and sensitivities, with SEs, across different definitions.
Materials and methods: We used retrospective queries of hospitalizations (2002-2011) in the Indiana Network for Patient Care with any CHF ICD-9 diagnoses, a primary diagnosis, an echocardiogram performed, a B-natriuretic peptide (BNP) drawn, or BNP >500 pg/mL. We used a hybrid between proportional sampling by Venn zone and over-sampling non-overlapping zones. The acute CHF (presence/absence) outcome was based on expert chart review using a priori criteria.
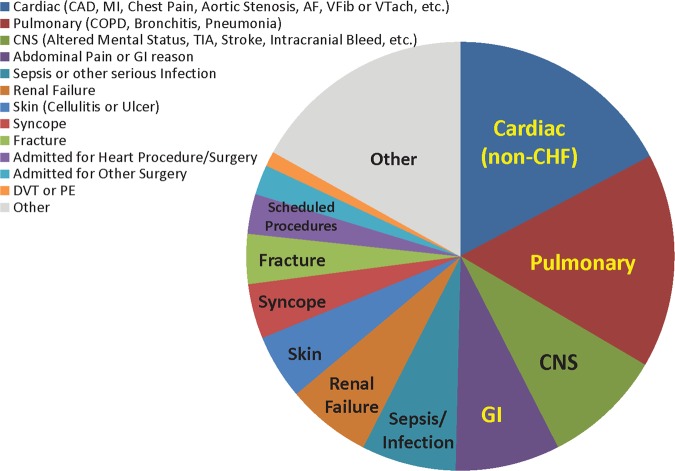
Results: Among 79,091 hospitalizations, we reviewed 908. A query for any ICD-9 code for CHF had PPV 42.8% (SE 1.5%) for acute CHF and sensitivity 94.3% (1.3%). Primary diagnosis of 428 and BNP >500 pg/mL had PPV 90.4% (SE 2.4%) and sensitivity 28.8% (1.1%). PPV was <10% when there was no echocardiogram, no BNP, and no primary diagnosis. 'False positive' hospitalizations were for other heart disease, lung disease, or other reasons.
Conclusions: This novel method successfully allowed flexible application and validation of queries for patients hospitalized with acute CHF.
Keywords: Algorithms; Electronic Health Records; Heart Failure; Phenotypes; Predictive Value of Tests; Validation Studies.
Figures

Similar articles
-
Congestive heart failure in the United States: is there more than meets the I(CD code)? The Corpus Christi Heart Project.Arch Intern Med. 2000 Jan 24;160(2):197-202. doi: 10.1001/archinte.160.2.197. Arch Intern Med. 2000. PMID: 10647758
-
Uncovering heart failure in patients with a history of pulmonary disease: rationale for the early use of B-type natriuretic peptide in the emergency department.Acad Emerg Med. 2003 Mar;10(3):198-204. doi: 10.1111/j.1553-2712.2003.tb01990.x. Acad Emerg Med. 2003. PMID: 12615582
-
B-type natriuretic peptide and echocardiographic determination of ejection fraction in the diagnosis of congestive heart failure in patients with acute dyspnea.Chest. 2005 Jul;128(1):21-9. doi: 10.1378/chest.128.1.21. Chest. 2005. PMID: 16002911
-
Chinese medicine syndromes in congestive heart failure: A literature study and retrospective analysis of clinical cases.Chin J Integr Med. 2016 Oct;22(10):738-44. doi: 10.1007/s11655-015-2085-6. Epub 2016 Feb 23. Chin J Integr Med. 2016. PMID: 26906719 Review.
-
Validity of Acute Cardiovascular Outcome Diagnoses Recorded in European Electronic Health Records: A Systematic Review.Clin Epidemiol. 2020 Oct 14;12:1095-1111. doi: 10.2147/CLEP.S265619. eCollection 2020. Clin Epidemiol. 2020. PMID: 33116903 Free PMC article. Review.
Cited by
-
Comparison of Approaches for Heart Failure Case Identification From Electronic Health Record Data.JAMA Cardiol. 2016 Dec 1;1(9):1014-1020. doi: 10.1001/jamacardio.2016.3236. JAMA Cardiol. 2016. PMID: 27706470 Free PMC article.
-
Identifying heart failure using EMR-based algorithms.Int J Med Inform. 2018 Dec;120:1-7. doi: 10.1016/j.ijmedinf.2018.09.016. Epub 2018 Sep 19. Int J Med Inform. 2018. PMID: 30409334 Free PMC article.
-
Letter to the editor in response to "Risk prediction of delirium in hospitalized patients using machine learning: an implementation and prospective evaluation study".J Am Med Inform Assoc. 2021 Mar 1;28(3):664-665. doi: 10.1093/jamia/ocaa285. J Am Med Inform Assoc. 2021. PMID: 33325514 Free PMC article. No abstract available.
-
Accuracy of Electronic Health Record-Based Definitions for Patients with Heart Failure.Am J Med. 2025 Jul 18:S0002-9343(25)00435-8. doi: 10.1016/j.amjmed.2025.07.010. Online ahead of print. Am J Med. 2025. PMID: 40684967
-
Do electronic health record systems "dumb down" clinicians?J Am Med Inform Assoc. 2022 Dec 13;30(1):172-177. doi: 10.1093/jamia/ocac163. J Am Med Inform Assoc. 2022. PMID: 36099154 Free PMC article.
References
-
- Rice JP, Saccone NL, Rasmussen E. Definition of the phenotype. Adv Genet 2001:42:69–76 - PubMed
-
- Wojczynski MK, Tiwari HK. Defintion of phenotype. Adv Genet 2008;60:75–105 - PubMed
-
- Stang PE, Ryan PB, Racoosin JA, et al. Advancing the science for active surveillance: rationale and design for the Observational Medical Outcomes Partnership. Ann Intern Med 2010;153:600–6 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
