

Cutaneous manifestations of ESRD
- PMID: 24115194
- PMCID: PMC3878705
- DOI: 10.2215/CJN.05900513
Cutaneous manifestations of ESRD
Abstract
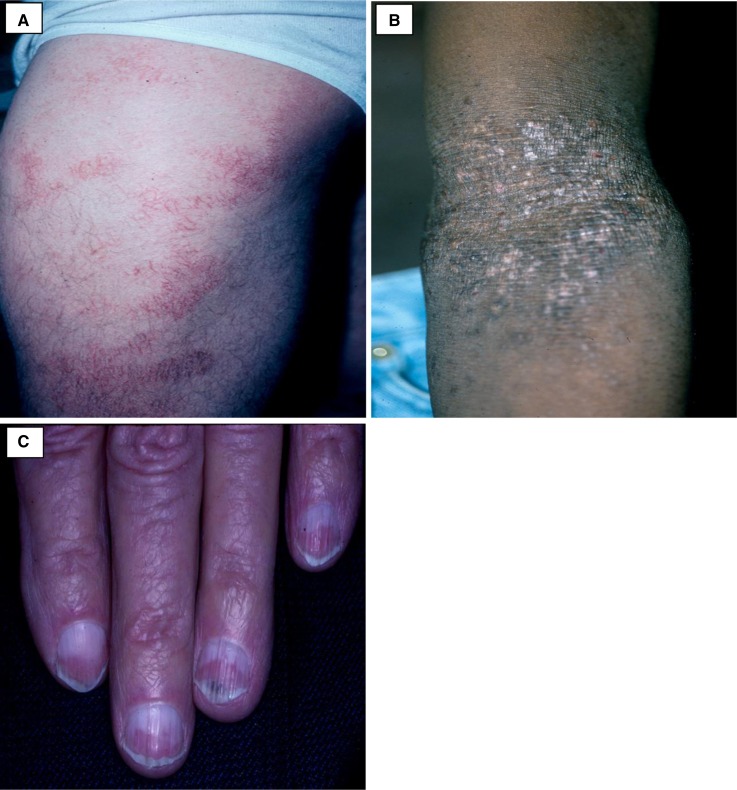
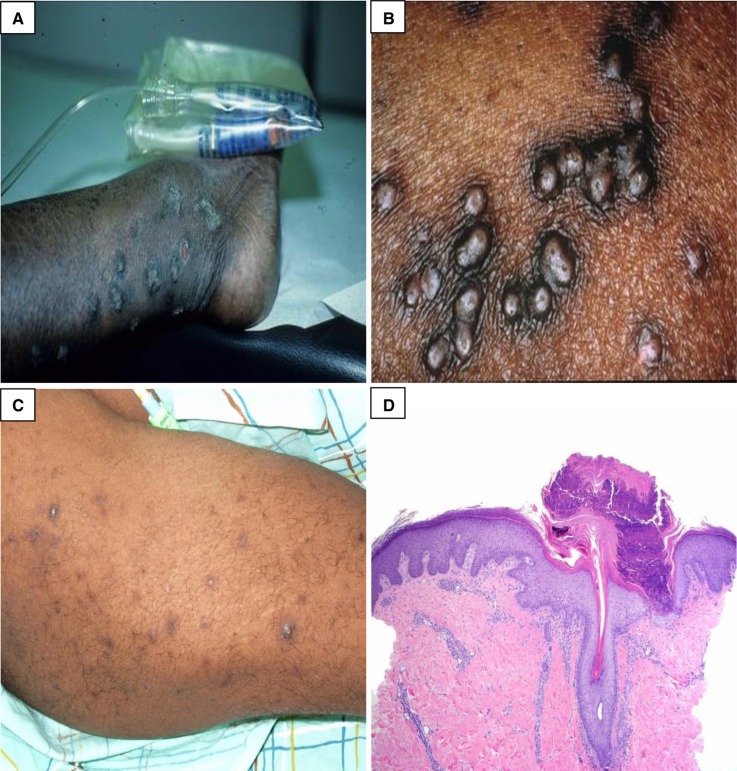
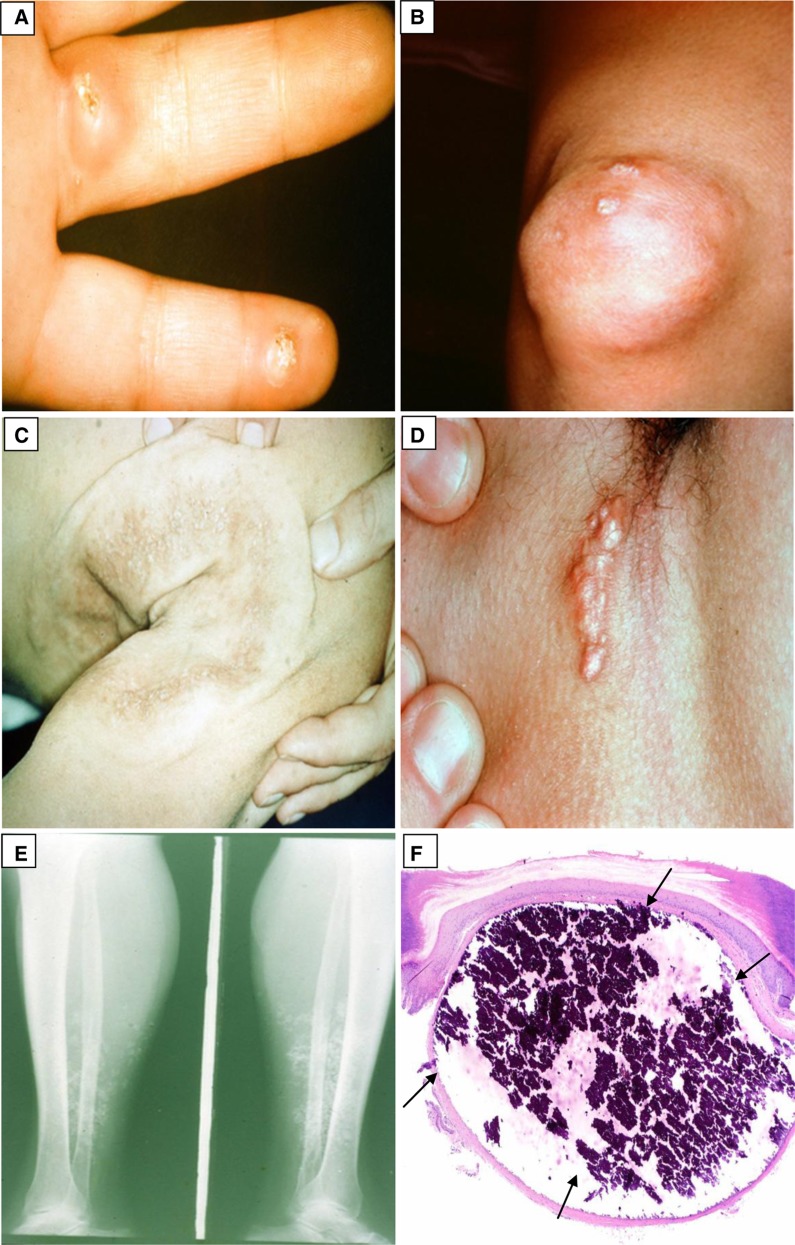
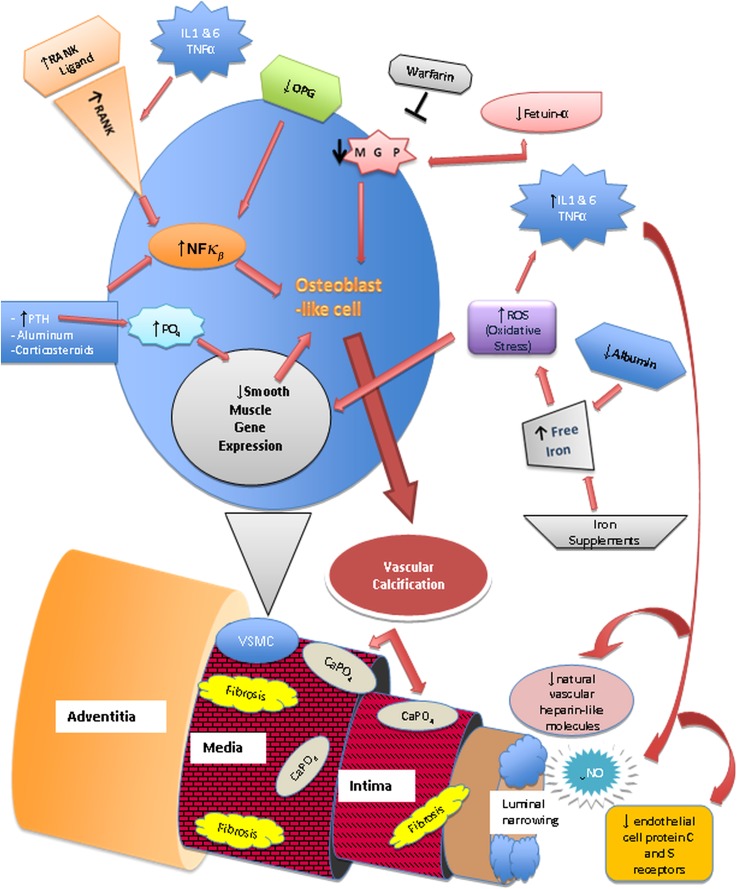
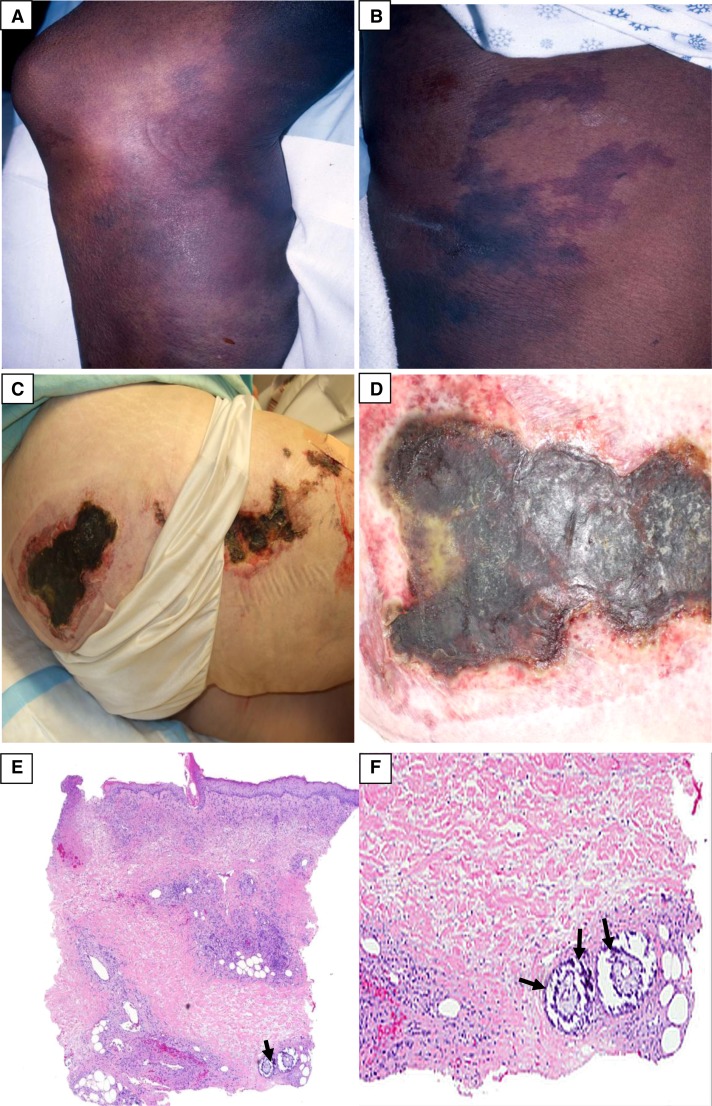
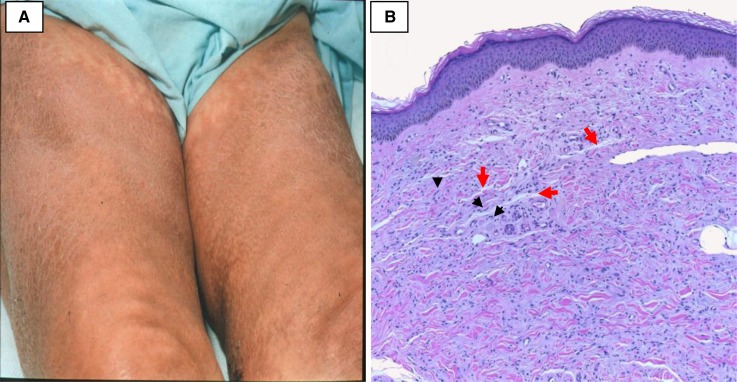
A broad range of skin diseases occurs in patients with ESRD: from the benign and asymptomatic to the physically disabling and life-threatening. Many of them negatively impact on quality of life. Their early recognition and treatment are essential in reducing morbidity and mortality. The cutaneous manifestations can be divided into two main categories: nonspecific and specific. The nonspecific manifestations are commonly seen and include skin color changes, xerosis, half-and-half nails, and pruritus. The specific disorders include acquired perforating dermatosis, bullous dermatoses, metastatic calcification, and nephrogenic systemic fibrosis. This review article describes these conditions and considers the underlying pathophysiology, clinical presentations, diagnosis, and treatment options.
Figures

References
-
- National Institutes of Health; National Institute of Diabetes and Digestive and Kidney Diseases; US Renal Data System: Annual Data Report: Atlas of Chronic Kidney Disease and End-Stage Renal Disease in the United States, 2012. Available at: http://www.usrds.org/2012/pdf/v2_ch1_12.pdf Accessed April 10, 2013
-
- Goldman, L, Schafer AI : Chronic Kidney Disease. In: Goldman’s Cecil Medicine, Expert Consult Premium Edition, 24th Ed., Philadelphia, Elsevier Saunders, 2012
-
- Attia EA, Hassan SI, Youssef NM: Cutaneous disorders in uremic patients on hemodialysis: An Egyptian case-controlled study. Int J Dermatol 49: 1024–1030, 2010 - PubMed
-
- Markova A, Lester J, Wang J, Robinson-Bostom L: Diagnosis of common dermopathies in dialysis patients: A review and update. Semin Dial 25: 408–418, 2012 - PubMed
-
- Airaghi L, Garofalo L, Cutuli MG, Delgado R, Carlin A, Demitri MT, Badalamenti S, Graziani G, Lipton JM, Catania A: Plasma concentrations of alpha-melanocyte-stimulating hormone are elevated in patients on chronic haemodialysis. Nephrol Dial Transplant 15: 1212–1216, 2000 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
