

Psychosocial intervention improves depression, quality of life, and fluid adherence in hemodialysis
- PMID: 24115478
- PMCID: PMC3871769
- DOI: 10.1681/ASN.2012111134
Psychosocial intervention improves depression, quality of life, and fluid adherence in hemodialysis
Abstract
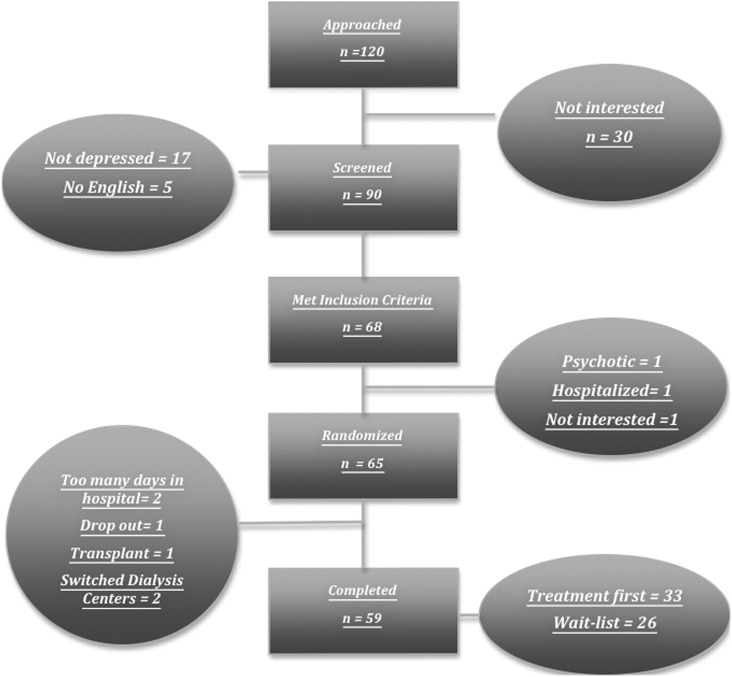
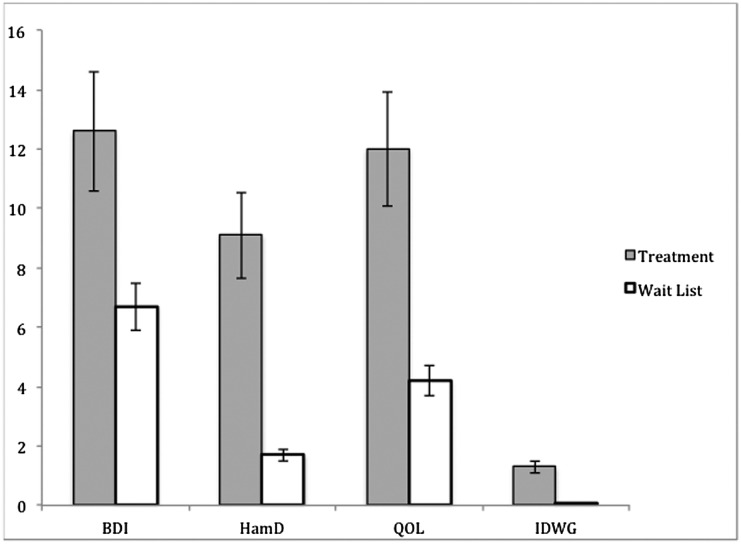
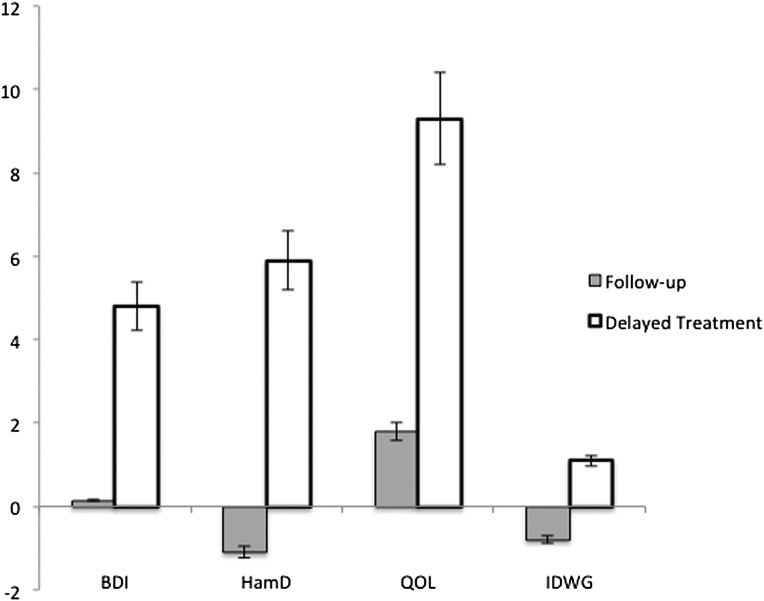
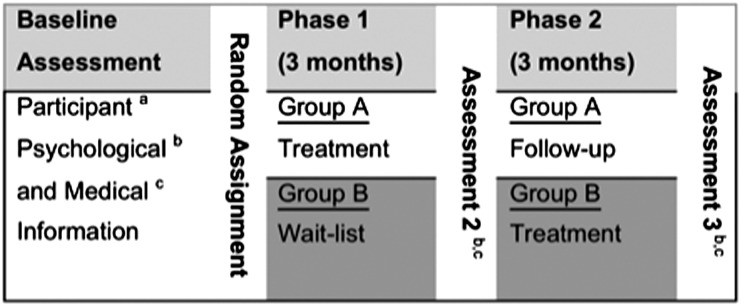
Patients with ESRD have high rates of depression, which is associated with diminished quality of life and survival. We determined whether individual cognitive behavioral therapy (CBT) reduces depression in hemodialysis patients with elevated depressive affect in a randomized crossover trial. Of 65 participants enrolled from two dialysis centers in New York, 59 completed the study and were assigned to the treatment-first group (n=33) or the wait-list control group (n=26). In the intervention phase, CBT was administered chairside during dialysis treatments for 3 months; participants were assessed 3 and 6 months after randomization. Compared with the wait-list group, the treatment-first group achieved significantly larger reductions in Beck Depression Inventory II (self-reported, P=0.03) and Hamilton Depression Rating Scale (clinician-reported, P<0.001) scores after intervention. Mean scores for the treatment-first group did not change significantly at the 3-month follow-up. Among participants with depression diagnosed at baseline, 89% in the treatment-first group were not depressed at the end of treatment compared with 38% in the wait-list group (Fisher's exact test, P=0.01). Furthermore, the treatment-first group experienced greater improvements in quality of life, assessed with the Kidney Disease Quality of Life Short Form (P=0.04), and interdialytic weight gain (P=0.002) than the wait-list group, although no effect on compliance was evident at follow-up. In summary, CBT led to significant improvements in depression, quality of life, and prescription compliance in this trial, and studies should be undertaken to assess the long-term effects of CBT on morbidity and mortality in patients with ESRD.
Figures
References
-
- Cukor D, Cohen SD, Peterson RA, Kimmel PL: Psychosocial aspects of chronic disease: ESRD as a paradigmatic illness. J Am Soc Nephrol 18: 3042–3055, 2007 - PubMed
-
- Kimmel PL: Psychosocial factors in dialysis patients. Kidney Int 59: 1599–1613, 2001 - PubMed
-
- Finkelstein FO, Finkelstein SH: Depression in chronic dialysis patients: Assessment and treatment. Nephrol Dial Transplant 15: 1911–1913, 2000 - PubMed
-
- Hedayati SS, Bosworth HB, Kuchibhatla M, Kimmel PL, Szczech LA: The predictive value of self-report scales compared with physician diagnosis of depression in hemodialysis patients. Kidney Int 69: 1662–1668, 2006 - PubMed
-
- Watnick S, Wang PL, Demadura T, Ganzini L: Validation of 2 depression screening tools in dialysis patients. Am J Kidney Dis 46: 919–924, 2005 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
