

Myasthenia gravis: an update for the clinician
- PMID: 24117026
- PMCID: PMC3927901
- DOI: 10.1111/cei.12217
Myasthenia gravis: an update for the clinician
Abstract
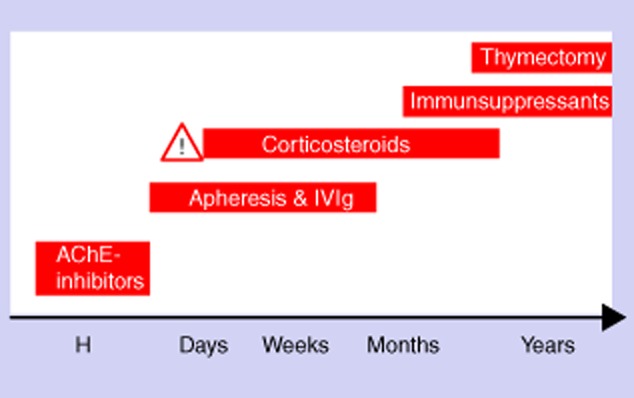
This paper provides a thorough overview of the current advances in diagnosis and therapy of myasthenia gravis (MG). Nowadays the term 'myasthenia gravis' includes heterogeneous autoimmune diseases, with a postsynaptic defect of neuromuscular transmission as the common feature. Myasthenia gravis should be classified according to the antibody specificity [acetylcholine, muscle-specific receptor tyrosine kinase (MuSK), low-density lipoprotein receptor-related protein 4 (LRP4), seronegative], thymus histology (thymitis, thymoma, atrophy), age at onset (in children; aged less than or more than 50 years) and type of course (ocular or generalized). With optimal treatment, the prognosis is good in terms of daily functions, quality of life and survival. Symptomatic treatment with acetylcholine esterase inhibition is usually combined with immunosuppression. Azathioprine still remains the first choice for long-term immunosuppressive therapy. Alternative immunosuppressive options to azathioprine include cyclosporin, cyclophosphamide, methotrexate, mycophenolate mofetil and tacrolimus. Rituximab is a promising new drug for severe generalized MG. Emerging therapy options include belimumab, eculizumab and the granulocyte- macrophage colony-stimulating factor. One pilot study on etanercept has given disappointing results. For decades, thymectomy has been performed in younger adults to improve non-paraneoplastic MG. However, controlled prospective studies on the suspected benefit of this surgical procedure are still lacking. In acute exacerbations, including myasthenic crisis, intravenous immunoglobulin, plasmapheresis and immunoadsorption are similarly effective.
Keywords: diagnostics; myasthenia gravis; neuroimmunology; therapy/immunotherapy.
© 2013 British Society for Immunology.
Figures
References
-
- Pakzad Z, Aziz T, Oger J. Increasing incidence of myasthenia gravis among elderly in British Columbia, Canada. Neurology. 2011;76:1526–1528. - PubMed
-
- Pallaver F, Riviera AP, Piffer S, et al. Change in myasthenia gravis epidemiology in Trento, Italy, after twenty years. Neuroepidemiology. 2011;36:282–287. - PubMed
-
- Matsuda M, Dohi-Iijima N, Nakamura A, et al. Increase in incidence of elderly-onset patients with myasthenia gravis in Nagano Prefecture, Japan. Intern Med. 2005;44:572–577. - PubMed
-
- Zivkovic SA, Clemens PR, Lacomis D. Characteristics of late-onset myasthenia gravis. J Neurol. 2012;259:2167–2171. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
