

Accountable Care Organizations in the United States: market and demographic factors associated with formation
- PMID: 24117222
- PMCID: PMC3876396
- DOI: 10.1111/1475-6773.12102
Accountable Care Organizations in the United States: market and demographic factors associated with formation
Abstract
Background: The Accountable Care Organization (ACO) model is rapidly being implemented by Medicare, private payers, and states, but little is known about the scope of ACO implementation.
Objective: To determine the number of accountable care organizations in the United States, where they are located, and characteristics associated with ACO formation.
Study design, methods, and data: Cross-sectional study of all ACOs in the United States as of August 2012. We identified ACOs from multiple sources; documented service locations (practices, clinics, hospitals); and linked service locations to local areas, defined as Dartmouth Atlas hospital service areas. We used multivariate analysis to assess what characteristics were associated with local ACO presence. We examined demographic characteristics (2010 American Community Survey) and health care system characteristics (2010 Medicare fee-for-service claims data).
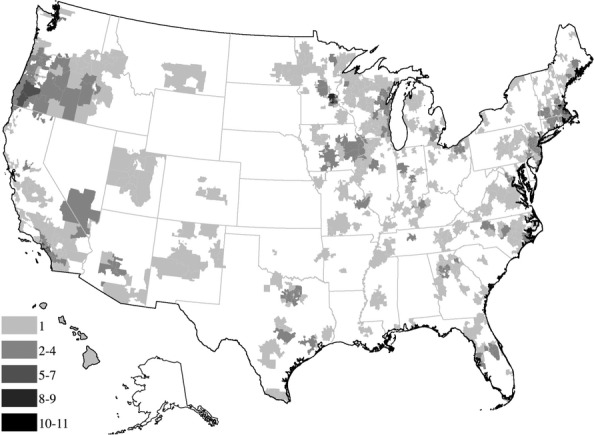
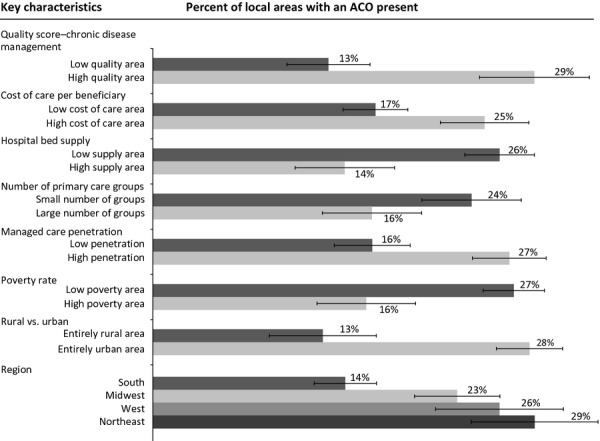
Principal findings: We identified 227 ACOs located in 27 percent of local areas. Fifty-five percent of the US population resides in these areas. HSA-level characteristics associated with ACO presence include higher performance on quality, higher Medicare per capita spending, fewer primary care physician groups, greater managed care penetration, lower poverty rates, and urban location.
Conclusions: Much of the US population resides in areas where ACOs have been established. ACO formation has taken place where it may be easier to meet quality and cost targets. Wider adoption of the ACO model may require tailoring to local context.
Keywords: Accountable care organizations; Medicare; delivery of health care; health care costs; health care reform; health policy; incentives in health care.
© Health Research and Educational Trust.
Figures
References
-
- Baker LC. “Association of Managed Care Market Share and Health Expenditures for Fee-for-Service Medicare Patients”. Journal of the American Medical Association. 1999;281(5):432–7. doi: 10.1001/jama.281.5.432. - DOI - PubMed
-
- Berenson RA, Ginsburg PB, Kemper N. “Unchecked Provider Clout in California Foreshadows Challenges to Health Reform”. Health Affairs. 2010;29(4):699–705. doi: 10.1377/hlthaff.2009.0715. - DOI - PubMed
-
- Berenson RA, Ginsburg PB, Christianson JB, Yee T. “The Growing Power of Some Providers to Win Steep Payment Increases from Insurers Suggests Policy Remedies May Be Needed”. Health Affairs. 2012;31(5):973–81. doi: 10.1377/hlthaff.2011.0920. - DOI - PubMed
-
- Berwick DM. “Making Good on ACOs' Promise—The Final Rule for the Medicare Shared Savings Program”. New England Journal of Medicine. 2011;365(19):1753–6. doi: 10.1056/NEJMp1111671. - DOI - PubMed
-
- Berwick DM, Hackbarth AD. “Eliminating Waste in US Health Care”. Journal of the American Medical Association. 2012;307(14):1513–6. doi: 10.1001/jama.2012.362. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
