

Myocardial Infarction - Stress PRevention INTervention (MI-SPRINT) to reduce the incidence of posttraumatic stress after acute myocardial infarction through trauma-focused psychological counseling: study protocol for a randomized controlled trial
- PMID: 24119487
- PMCID: PMC3852224
- DOI: 10.1186/1745-6215-14-329
Myocardial Infarction - Stress PRevention INTervention (MI-SPRINT) to reduce the incidence of posttraumatic stress after acute myocardial infarction through trauma-focused psychological counseling: study protocol for a randomized controlled trial
Abstract
Background: Posttraumatic Stress Disorder (PTSD) may occur in patients after exposure to a life-threatening illness. About one out of six patients develop clinically relevant levels of PTSD symptoms after acute myocardial infarction (MI). Symptoms of PTSD are associated with impaired quality of life and increase the risk of recurrent cardiovascular events. The main hypothesis of the MI-SPRINT study is that trauma-focused psychological counseling is more effective than non-trauma focused counseling in preventing posttraumatic stress after acute MI.
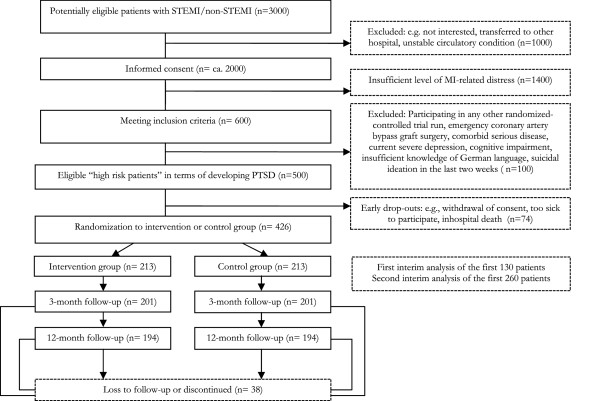
Methods/design: The study is a single-center, randomized controlled psychological trial with two active intervention arms. The sample consists of 426 patients aged 18 years or older who are at 'high risk' to develop clinically relevant posttraumatic stress symptoms. 'High risk' patients are identified with three single-item questions with a numeric rating scale (0 to 10) asking about 'pain during MI', 'fear of dying until admission' and/or 'worrying and feeling helpless when being told about having MI'. Exclusion criteria are emergency heart surgery, severe comorbidities, current severe depression, disorientation, cognitive impairment and suicidal ideation. Patients will be randomly allocated to a single 45-minute counseling session targeting either specific MI-triggered traumatic reactions (that is, the verum intervention) or the general role of psychosocial stress in coronary heart disease (that is, the control intervention). The session will take place in the coronary care unit within 48 hours, by the bedside, after patients have reached stable circulatory conditions. Each patient will additionally receive an illustrated information booklet as study material. Sociodemographic factors, psychosocial and medical data, and cardiometabolic risk factors will be assessed during hospitalization. The primary outcome is the interviewer-rated posttraumatic stress level at three-month follow-up, which is hypothesized to be at least 20% lower in the verum group than in the control group using the t-test. Secondary outcomes are posttraumatic stress levels at 12-month follow-up, and psychosocial functioning and cardiometabolic risk factors at both follow-up assessments.
Discussion: If the verum intervention proves to be effective, the study will be the first to show that a brief trauma-focused psychological intervention delivered within a somatic health care setting can reduce the incidence of posttraumatic stress in acute MI patients.
Trial registration: ClinicalTrials.gov: NCT01781247.
Figures
References
-
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 4. Washington DC: APA; 1994.
-
- Schelling G. Post-traumatic stress disorder in somatic disease: lessons from critically ill patients. Prog Brain Res. 2008;167:229–237. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
