

Randomized trial of preoperative docetaxel with or without capecitabine after 4 cycles of 5-fluorouracil– epirubicin–cyclophosphamide (FEC) in early-stage breast cancer: exploratory analyses identify Ki67 as a predictive biomarker for response to neoadjuvant chemotherapy
- PMID: 24122389
- PMCID: PMC3825616
- DOI: 10.1007/s10549-013-2691-y
Randomized trial of preoperative docetaxel with or without capecitabine after 4 cycles of 5-fluorouracil– epirubicin–cyclophosphamide (FEC) in early-stage breast cancer: exploratory analyses identify Ki67 as a predictive biomarker for response to neoadjuvant chemotherapy
Abstract
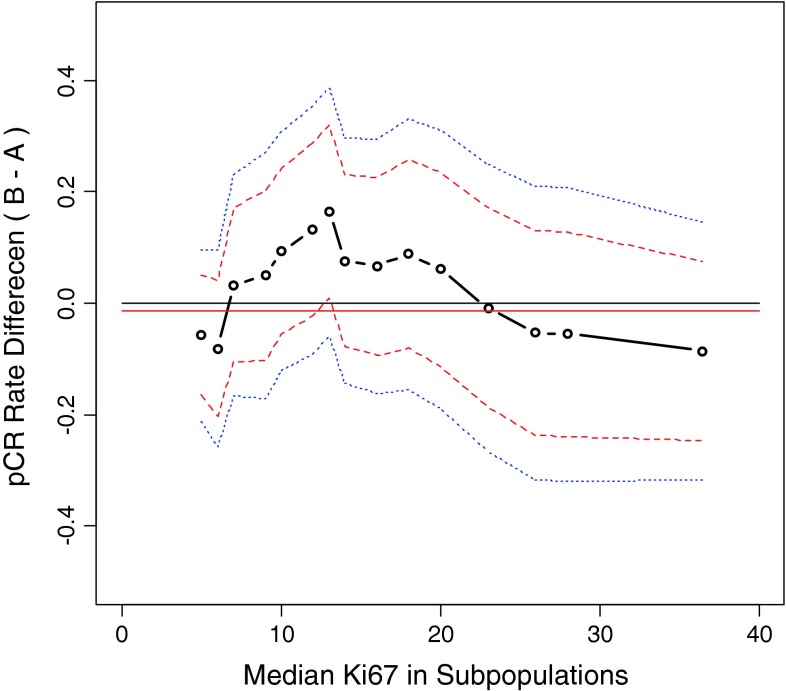
This randomized, multicenter study compared the efficacy of docetaxel with or without capecitabine following fluorouracil/epirubicin/cyclophosphamide (FEC) therapy in operable breast cancer and investigated the role of Ki67 as a predictive biomarker. Patients were randomized to 4 cycles of docetaxel/capecitabine (docetaxel: 75 mg/m2 on day 1; capecitabine: 1,650 mg/m2 on days 1–14 every 3 weeks) or docetaxel alone (75 mg/m2 on day 1 every 3 weeks) after completion of 4 cycles of FEC (5-fluorouracil 500 mg/m2, epirubicin 100 mg/m2 and cyclophosphamide 500 mg/m2 on day 1 every 3 weeks). The primary endpoint was the pathological complete response (pCR) rate. Predictive factor analysis was conducted using clinicopathological markers, including hormone receptors and Ki67 labeling index (Ki67LI). A total of 477 patients were randomized; the overall response in the docetaxel/capecitabine and docetaxel groups was 88.3 and 87.4 %, respectively. There were no significant differences in the pCR rate (docetaxel/capecitabine: 23 %; docetaxel: 24 %; p = 0.748), disease-free survival, or overall survival. However, patients with mid-range Ki67LI (10–20 %) showed a trend towards improved pCR rate with docetaxel/capecitabine compared to docetaxel alone. Furthermore, multivariate logistic regression analysis showed pre-treatment Ki67LI (odds ratio 1.031; 95 % CI 1.014–1.048; p = 0.0004) to be a significant predictor of pCR in this neoadjuvant treatment setting. Docetaxel/capecitabine (after 4 cycles of FEC) did not generate significant improvement in pCR compared to docetaxel alone. However, exploratory analyses suggested that assessment of pre-treatment Ki67LI may be a useful tool in the identification of responders to preoperative docetaxel/capecitabine in early-stage breast cancer.
Figures


References
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
