

HIV and the risk of direct obstetric complications: a systematic review and meta-analysis
- PMID: 24124458
- PMCID: PMC3790789
- DOI: 10.1371/journal.pone.0074848
HIV and the risk of direct obstetric complications: a systematic review and meta-analysis
Abstract
Background: Women of reproductive age in parts of sub-Saharan Africa are faced both with high levels of HIV and the threat of dying from the direct complications of pregnancy. Clinicians practicing in such settings have reported a high incidence of direct obstetric complications among HIV-infected women, but the evidence supporting this is unclear. The aim of this systematic review is to establish whether HIV-infected women are at increased risk of direct obstetric complications.
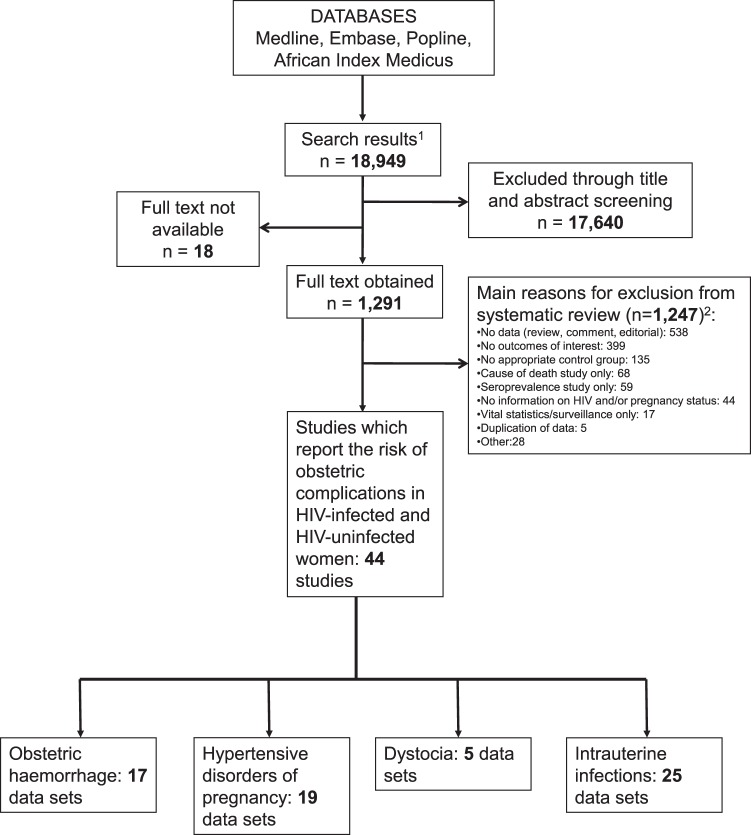
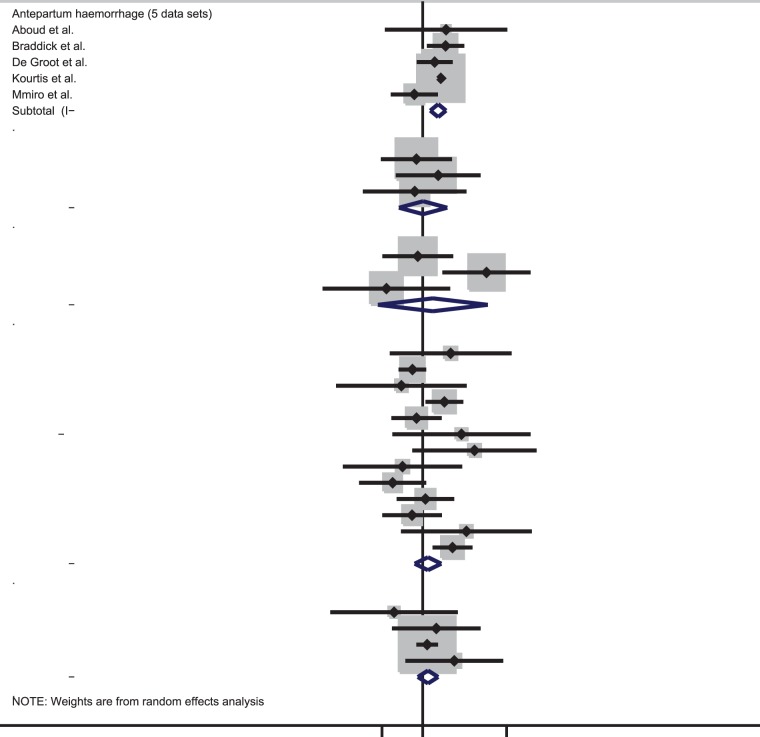
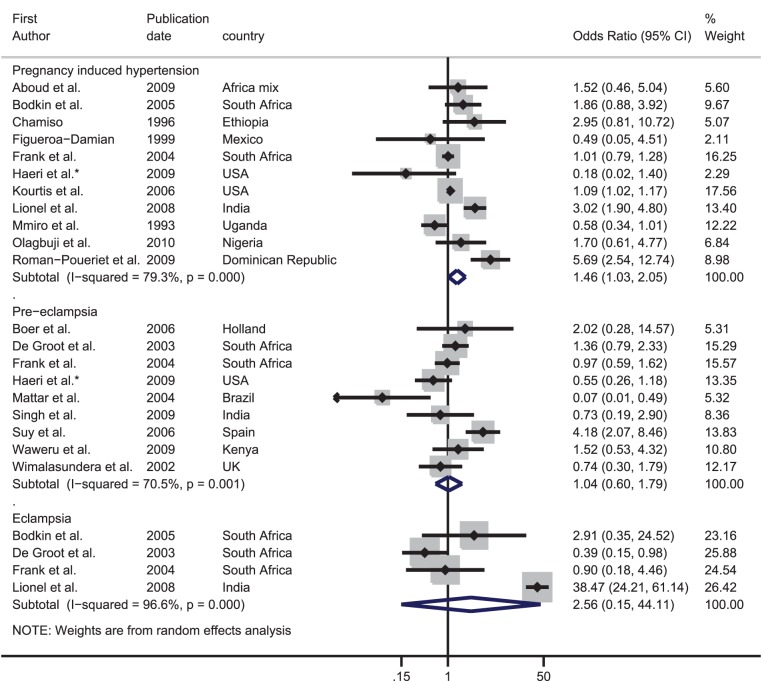
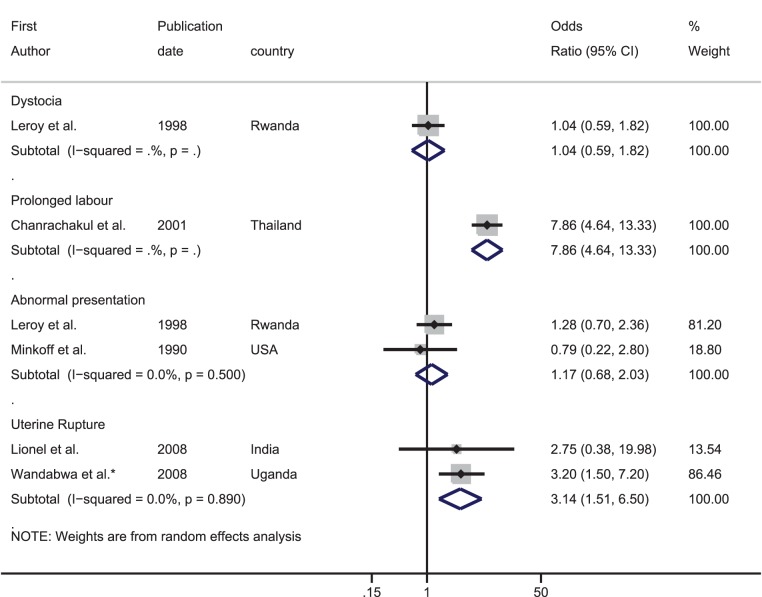
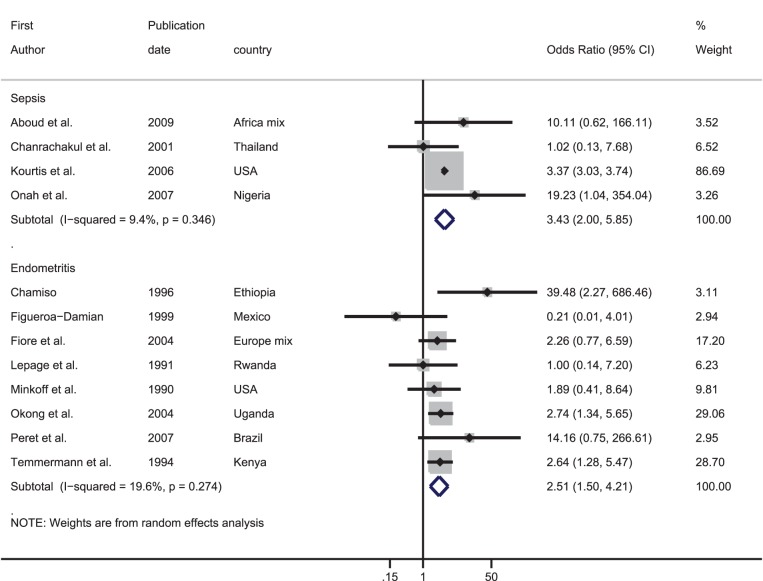
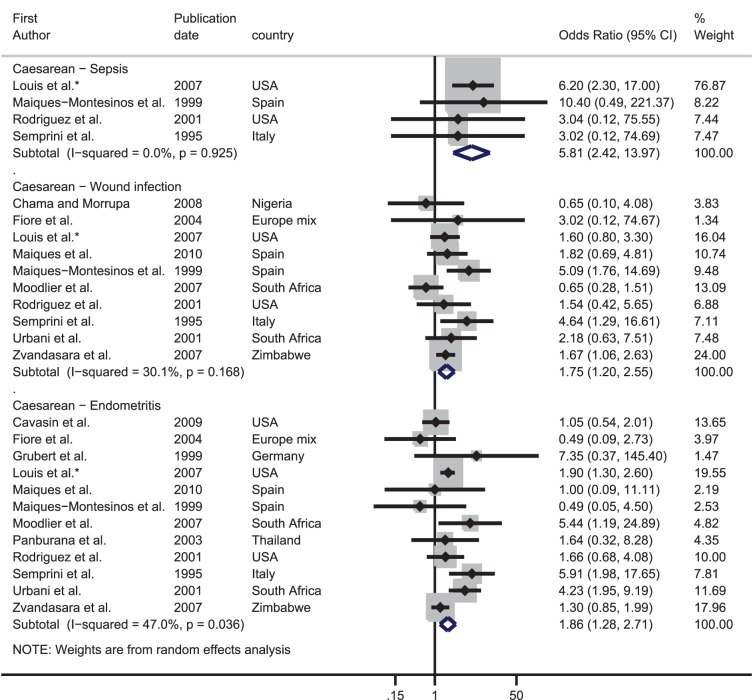
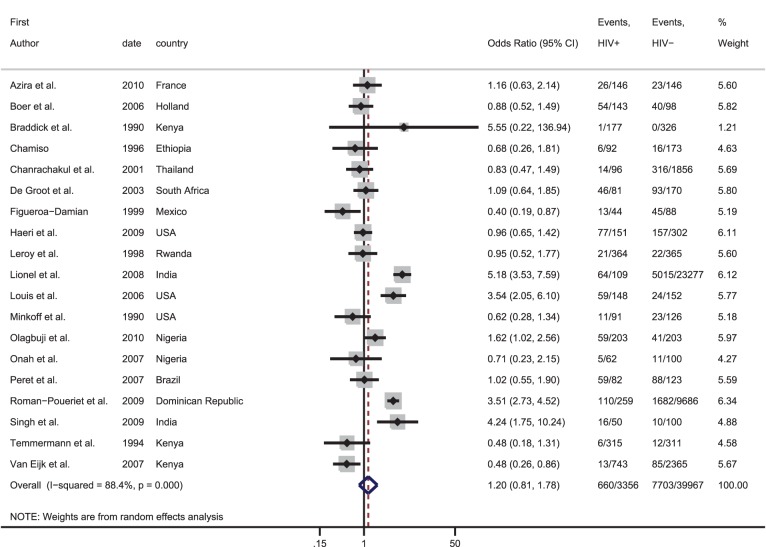
Methods and findings: Studies comparing the frequency of obstetric haemorrhage, hypertensive disorders of pregnancy, dystocia and intrauterine infections in HIV-infected and uninfected women were identified. Summary estimates of the odds ratio (OR) for the association between HIV and each obstetric complication were calculated through meta-analyses. In total, 44 studies were included providing 66 data sets; 17 on haemorrhage, 19 on hypertensive disorders, five on dystocia and 25 on intrauterine infections. Meta-analysis of the OR from studies including vaginal deliveries indicated that HIV-infected women had over three times the risk of a puerperal sepsis compared with HIV-uninfected women [pooled OR: 3.43, 95% confidence interval (CI): 2.00-5.85]; this figure increased to nearly six amongst studies only including women who delivered by caesarean (pooled OR: 5.81, 95% CI: 2.42-13.97). For other obstetric complications the evidence was weak and inconsistent.
Conclusions: The higher risk of intrauterine infections in HIV-infected pregnant and postpartum women may require targeted strategies involving the prophylactic use of antibiotics during labour. However, as the huge excess of pregnancy-related mortality in HIV-infected women is unlikely to be due to a higher risk of direct obstetric complications, reducing this mortality will require non obstetric interventions involving access to ART in both pregnant and non-pregnant women.
Conflict of interest statement
Figures
References
-
- Abdool-Karim Q, AbouZahr C, Dehne K, Mangiaterra V, Moodley J, et al. (2010) HIV and maternal mortality: turning the tide. The Lancet 375: 1948–1949. - PubMed
-
- McIntyre J (2003) Mothers infected with HIV: Reducing maternal death and disability during pregnancy. British Medical Bulletin 67: 127–135. - PubMed
-
- Lindgren S, Martin C, Anzen B, Strand H, Bredberg-Raden U, et al. (1996) Pattern of HIV viraemia and CD4 levels in relation to pregnancy in HIV-1 infected women. Scand J Infect Dis 28: 425–433. - PubMed
-
- Rich KC, Siegel JN, Jennings C, Rydman RJ, Landay AL (1995) CD4+ lymphocytes in perinatal human immunodeficiency virus (HIV) infection: evidence for pregnancy-induced immune depression in uninfected and HIV-infected women. J Infect Dis 172: 1221–1227. - PubMed
-
- French R, Brocklehurst P (1998) The effect of pregnancy on survival in women infected with HIV a systematic review of the literature and meta-analysis. BJOG: An International Journal of Obstetrics & Gynaecology 105: 827–835. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
