

Hematopoietic cell transplantation-specific comorbidity index predicts inpatient mortality and survival in patients who received allogeneic transplantation admitted to the intensive care unit
- PMID: 24127454
- PMCID: PMC4878009
- DOI: 10.1200/JCO.2013.50.5867
Hematopoietic cell transplantation-specific comorbidity index predicts inpatient mortality and survival in patients who received allogeneic transplantation admitted to the intensive care unit
Abstract
Purpose: To investigate the prognostic value of the Hematopoietic Cell Transplantation-Specific Comorbidity Index (HCT-CI) in patients who received transplantation admitted to the intensive care unit (ICU).
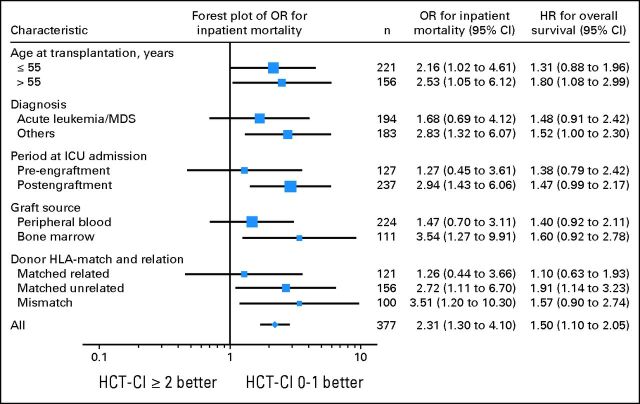
Patients and methods: We investigated the association of HCT-CI with inpatient mortality and overall survival (OS) among 377 patients who were admitted to the ICU within 100 days of allogeneic stem-cell transplantation (ASCT) at our institution. HCT-CI scores were collapsed into four groups and were evaluated in univariate and multivariate analyses using logistic regression and Cox proportional hazards models.
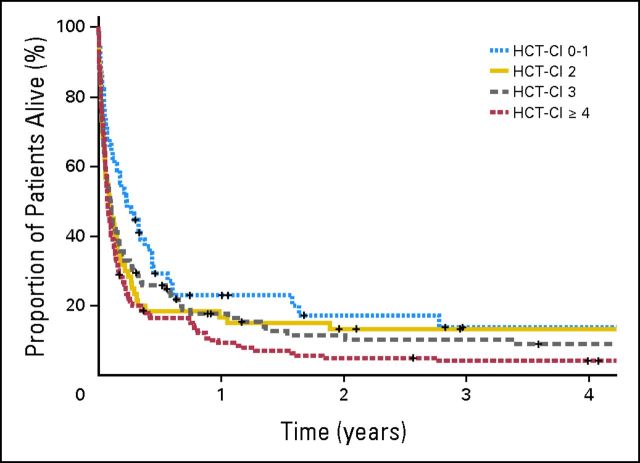
Results: The most common pretransplantation comorbidities were pulmonary and cardiac diseases, and respiratory failure was the primary reason for ICU admission. We observed a strong trend for higher inpatient mortality and shorter OS among patients with HCT-CI values ≥ 2 compared with patients with values of 0 to 1 in all patient subsets studied. Multivariate analysis showed that patients with HCT-CI values ≥ 2 had significantly higher inpatient mortality than patients with values of 0 to 1 and that HCT-CI values ≥ 4 were significantly associated with shorter OS compared with values of 0 to 1 (hazard ratio, 1.74; 95% CI, 1.23 to 2.47). The factors associated with lower inpatient mortality were ICU admission during the ASCT conditioning phase or the use of reduced-intensity conditioning regimens. The overall inpatient mortality rate was 64%, and the 1-year OS rate was 15%. Among patients with HCT-CI scores of 0 to 1, 2, 3, and ≥ 4, the 1-year OS rates were 22%, 17%, 18%, and 9%, respectively.
Conclusion: HCT-CI is a valuable predictor of mortality and survival in critically ill patients after ASCT.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest and author contributions are found at the end of this article.
Figures
References
-
- McArdle JR. Critical care outcomes in the hematologic transplant recipient. Clin Chest Med. 2009;30:155–167. - PubMed
-
- Afessa B, Tefferi A, Hoagland HC, et al. Outcome of recipients of bone marrow transplants who require intensive-care unit support. Mayo Clin Proc. 1992;67:117–122. - PubMed
-
- Soubani AO, Kseibi E, Bander JJ, et al. Outcome and prognostic factors of hematopoietic stem cell transplantation recipients admitted to a medical ICU. Chest. 2004;126:1604–1611. - PubMed
-
- Gilli K, Remberger M, Hjelmqvist H, et al. Sequential Organ Failure Assessment predicts the outcome of SCT recipients admitted to intensive care unit. Bone Marrow Transplant. 2010;45:682–688. - PubMed
-
- Jackson SR, Tweeddale MG, Barnett MJ, et al. Admission of bone marrow transplant recipients to the intensive care unit: Outcome, survival and prognostic factors. Bone Marrow Transplant. 1998;21:697–704. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
