

Transient regulatory T cell ablation deters oncogene-driven breast cancer and enhances radiotherapy
- PMID: 24127486
- PMCID: PMC3804934
- DOI: 10.1084/jem.20130762
Transient regulatory T cell ablation deters oncogene-driven breast cancer and enhances radiotherapy
Abstract
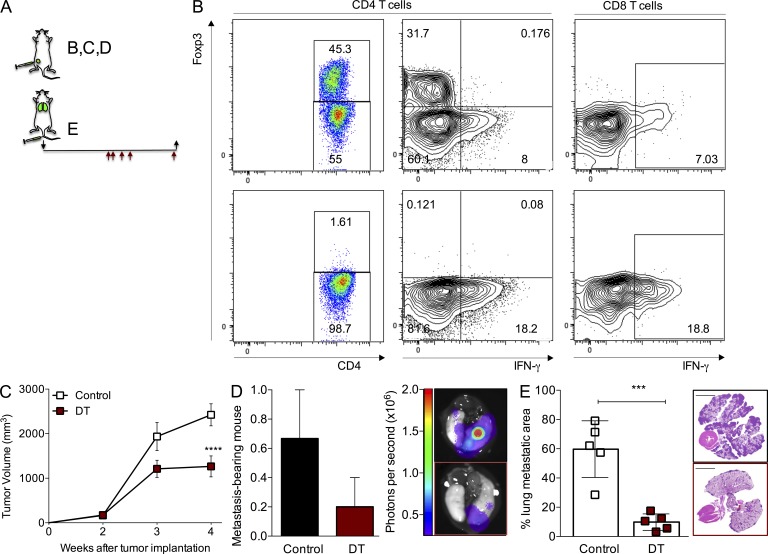
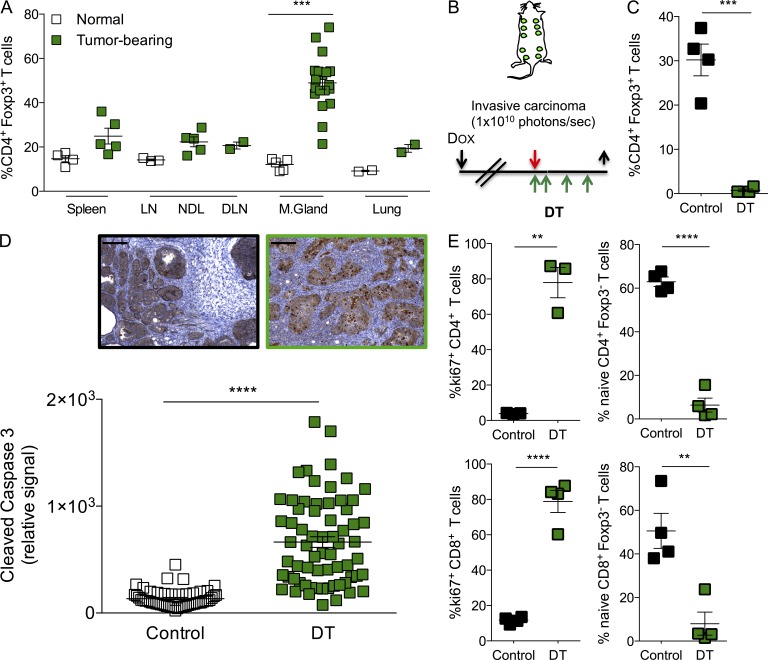
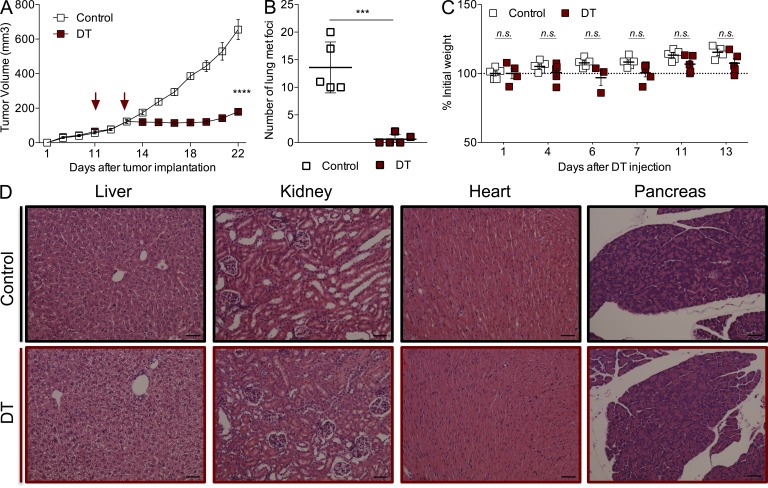
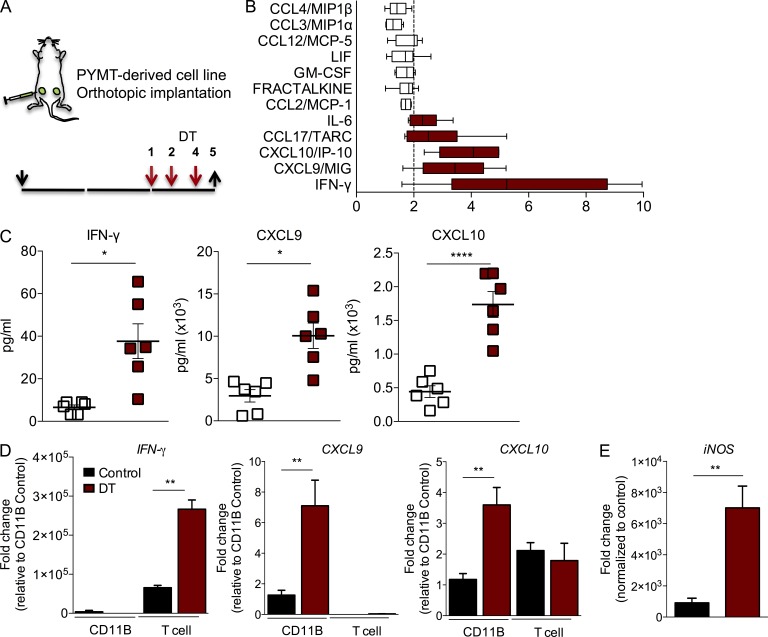
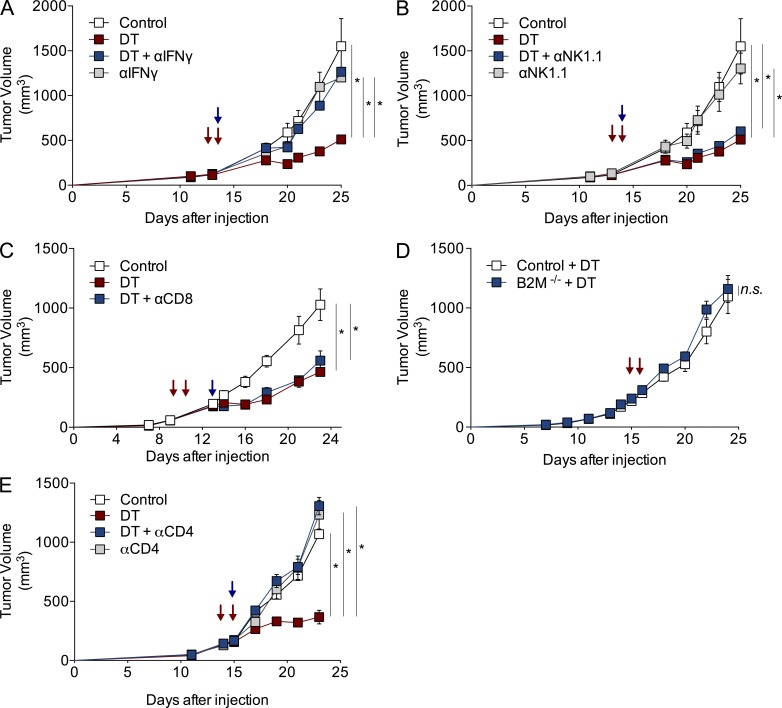
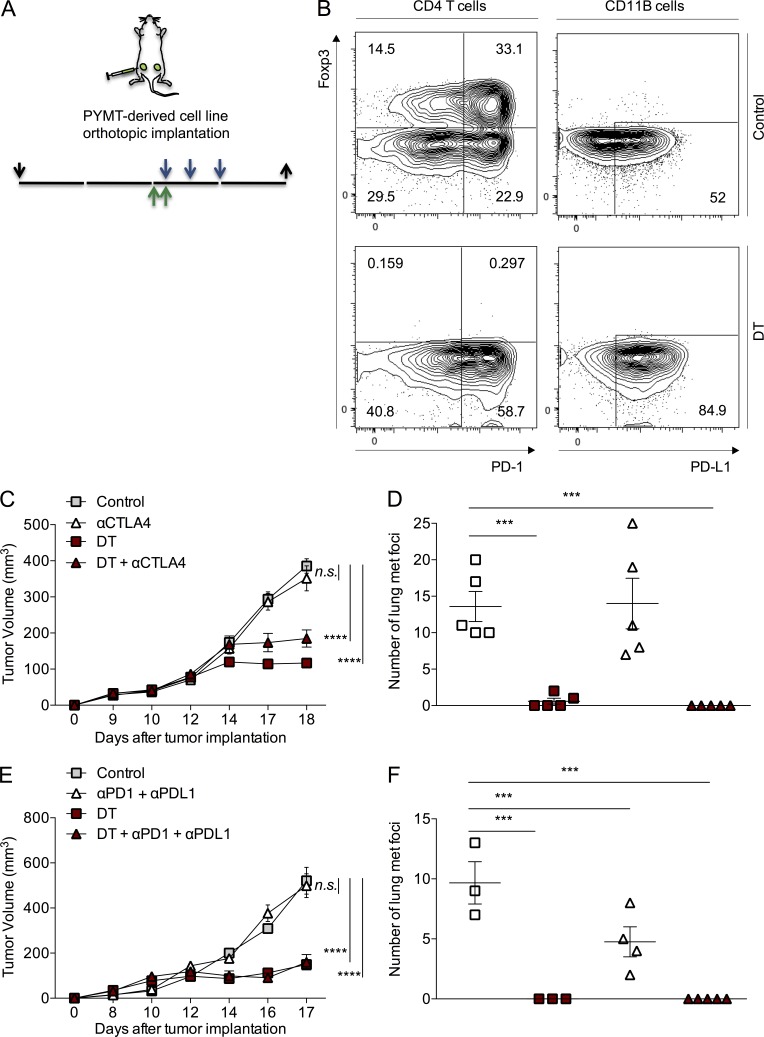
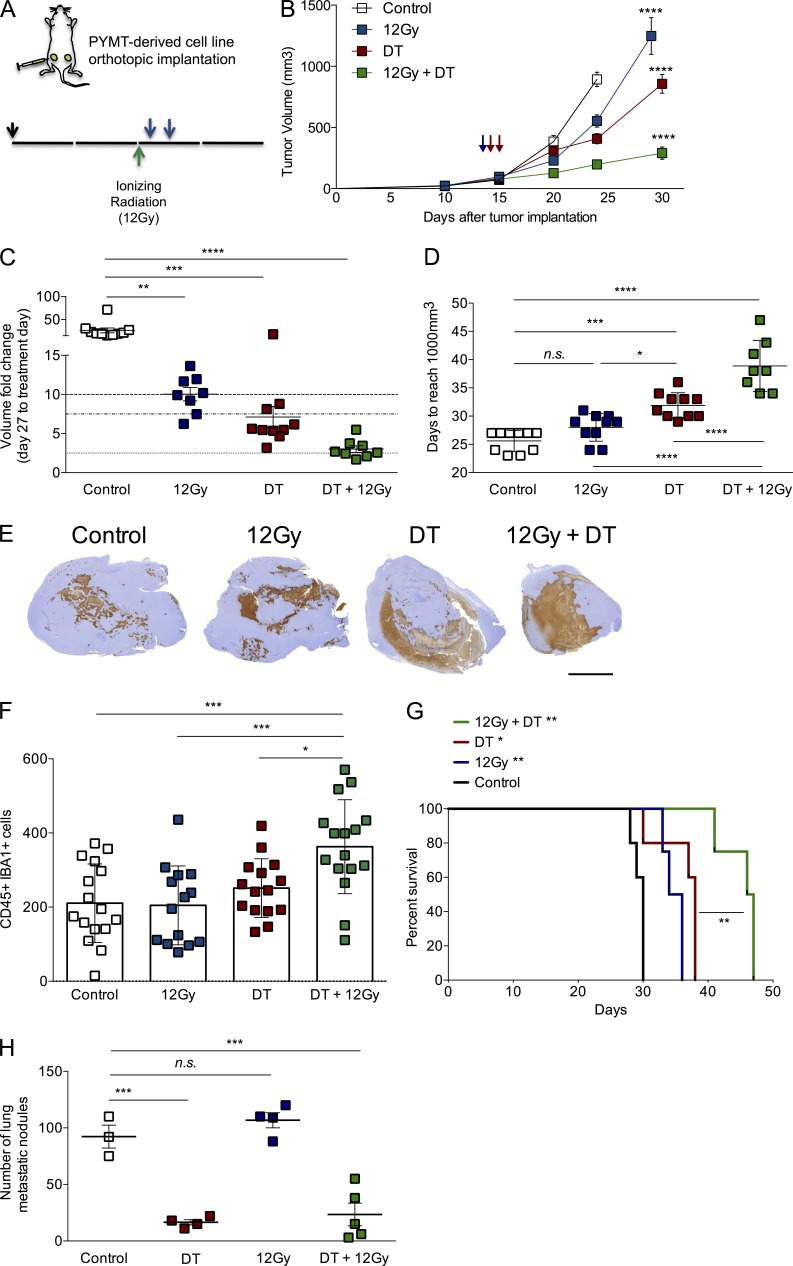
Rational combinatorial therapeutic strategies have proven beneficial for the management of cancer. Recent success of checkpoint blockade in highly immunogenic tumors has renewed interest in immunotherapy. Regulatory T (T reg) cells densely populate solid tumors, which may promote progression through suppressing anti-tumor immune responses. We investigated the role of T reg cells in murine mammary carcinogenesis using an orthotopic, polyoma middle-T antigen-driven model in Foxp3(DTR) knockin mice. T reg cell ablation resulted in significant determent of primary and metastatic tumor progression. Importantly, short-term ablation of T reg cells in advanced spontaneous tumors led to extensive apoptotic tumor cell death. This anti-tumor activity was dependent on IFN-γ and CD4(+) T cells but not on NK or CD8(+) T cells. Combination of T reg cell ablation with CTLA-4 or PD-1/PD-L1 blockade did not affect tumor growth or improve the therapeutic effect attained by T reg cell ablation alone. However, T reg cell targeting jointly with tumor irradiation significantly reduced tumor burden and improved overall survival. Together, our results demonstrate a major tumor-promoting role of T reg cells in an autochthonous model of tumorigenesis, and they reveal the potential therapeutic value of combining transient T reg cell ablation with radiotherapy for the management of poorly immunogenic, aggressive malignancies.
Figures
References
-
- Balachandran V.P., Cavnar M.J., Zeng S., Bamboat Z.M., Ocuin L.M., Obaid H., Sorenson E.C., Popow R., Ariyan C., Rossi F., et al. 2011. Imatinib potentiates antitumor T cell responses in gastrointestinal stromal tumor through the inhibition of Ido. Nat. Med. 17:1094–1100 10.1038/nm.2438 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Research Materials
