

Clinical, radiological, histological and molecular characteristics of paediatric epithelioid glioblastoma
- PMID: 24127995
- PMCID: PMC4042629
- DOI: 10.1111/nan.12093
Clinical, radiological, histological and molecular characteristics of paediatric epithelioid glioblastoma
Abstract
Aims: A few case series in adults have described the characteristics of epithelioid glioblastoma (e-GB), one of the rarest variants of this cancer. We evaluated clinical, radiological, histological and molecular characteristics in the largest series to date of paediatric e-GB.
Methods: Review of clinical characteristics and therapy, imaging studies and histology was performed in patients younger than 22 years with e-GB seen at our institution over 15 years. Sequencing of hotspot mutations and fluorescence in situ hybridization of relevant genes were undertaken.
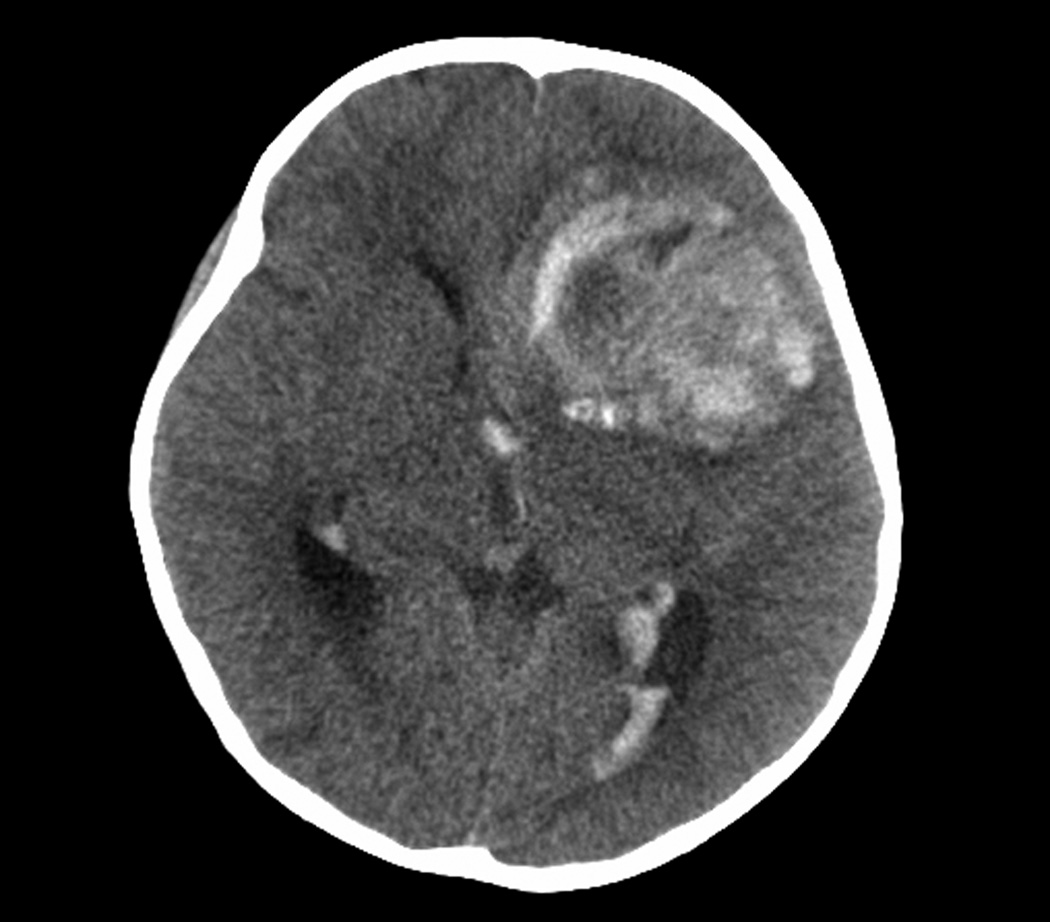
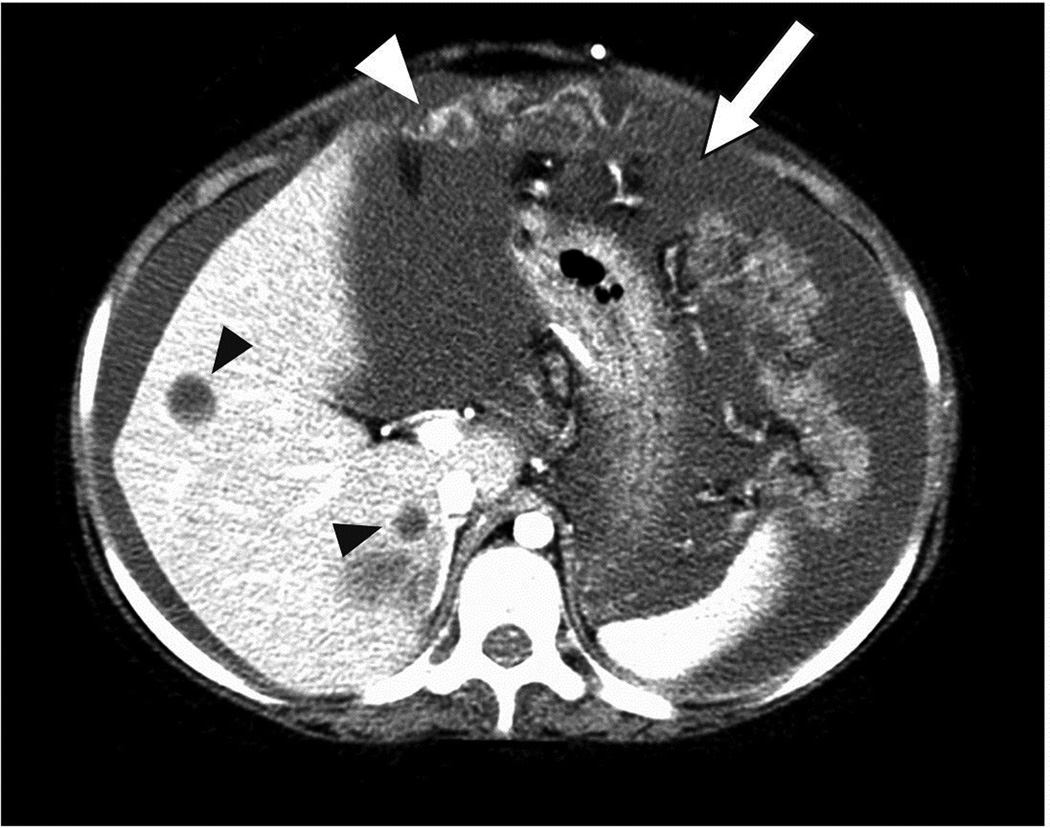
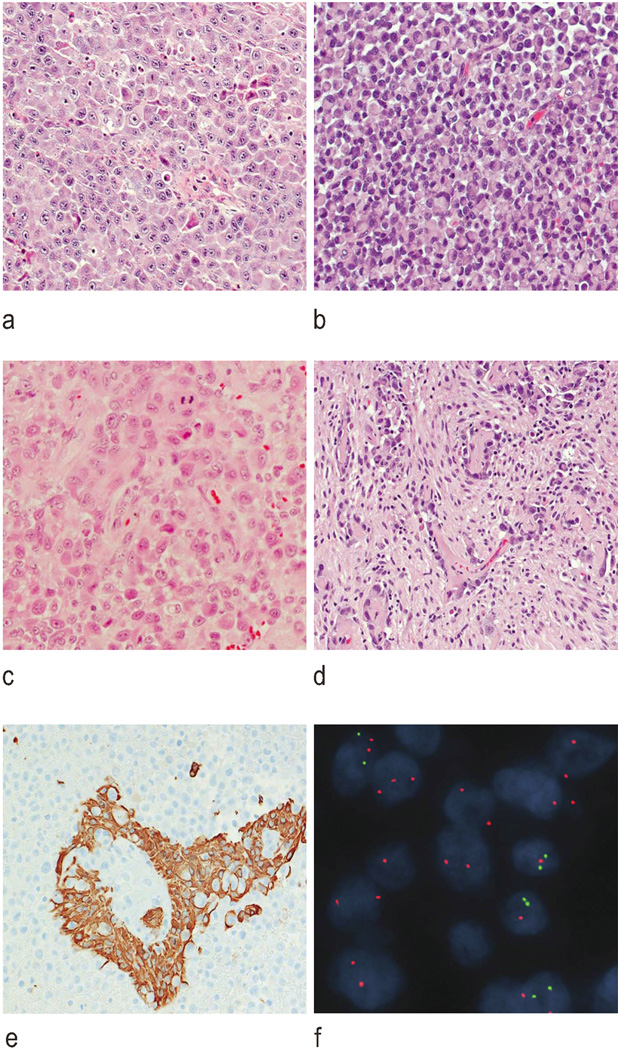
Results: Median age at diagnosis of six patients was 7.6 years. Tumours originated in the cerebral cortex (n = 2) or diencephalon (n = 4). Three patients presented with acute, massive haemorrhage and three had leptomeningeal dissemination at diagnosis. Paediatric e-GB had the typical histological characteristics seen in adult tumours. Universal immunoreactivity for INI1 and lack of diverse protein expression were seen in all cases. One tumour had a chromosome 22q loss. Three tumours (50%) harboured a BRAF: p.V600E. One thalamic tumour had an H3F3A p.K27M. All patients received radiation therapy with (n = 3) or without chemotherapy (n = 3). All patients experienced tumour progression with a median survival of 169 days. One patient with nonmetastatic disease had early leptomeningeal progression. Two patients had symptomatic tumour spread outside the central nervous system (CNS) through a ventriculoperitoneal shunt. One additional patient had widespread metastases outside the CNS identified at autopsy.
Conclusions: Paediatric e-GBs are rare cancers with an aggressive behaviour that share histological and genetic characteristics with their adult counterparts. BRAF inhibition is a potential treatment for these tumours.
Keywords: BRAF; epithelioid; glioblastoma; paediatric; rhabdoid.
© 2013 British Neuropathological Society.
Conflict of interest statement
Figures
References
-
- Kleihues P, Burger PC, Aldape KD, Brat DJ, Biernat W, Bigner DD, Nakazato Y, Plate KH, Giangaspero F, von Deimling A, Ohgaki H, Cavenee WK. Glioblastoma. In: Louis DN, Ohgaki H, Wiestler OD, Webster WK, editors. WHO Classification of Tumours of the Central Nervous System. 4th edn. Lyon: IARC Press; 2007. pp. 33–49.
-
- Kepes JJ, Fulling KH, Garcia JH. The clinical significance of“adenoid” formations of neoplastic astrocytes, imitating metastatic carcinoma, in gliosarcomas. A review of five cases. Clin Neuropathol. 1982;1:139–150. - PubMed
-
- Kornfeld M. Granular cell glioblastoma: a malignant granular cell neoplasm of astrocytic origin. J Neuropathol Exp Neurol. 1986;45:447–462. - PubMed
-
- Mørk SJ, Rubinstein LJ, Kepes JJ, Perentes E, Uphoff DF. Patterns of epithelial metaplasia in malignant gliomas. II. Squamous differentiation of epithelial-like formations in gliosarcomas and glioblastomas. J Neuropathol Exp Neurol. 1988;47:101–118. - PubMed
-
- Burger PC, Pearl DK, Aldape K, Yates AJ, Scheithauer BW, Passe SM, Jenkins RB, James CD. Small cell architecture--a histological equivalent of EGFR amplification in glioblastoma multiforme? J Neuropathol Exp Neurol. 2001;60:1099–1104. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
