

Increased survival in pancreatic cancer with nab-paclitaxel plus gemcitabine
- PMID: 24131140
- PMCID: PMC4631139
- DOI: 10.1056/NEJMoa1304369
Increased survival in pancreatic cancer with nab-paclitaxel plus gemcitabine
Abstract
Background: In a phase 1-2 trial of albumin-bound paclitaxel (nab-paclitaxel) plus gemcitabine, substantial clinical activity was noted in patients with advanced pancreatic cancer. We conducted a phase 3 study of the efficacy and safety of the combination versus gemcitabine monotherapy in patients with metastatic pancreatic cancer.
Methods: We randomly assigned patients with a Karnofsky performance-status score of 70 or more (on a scale from 0 to 100, with higher scores indicating better performance status) to nab-paclitaxel (125 mg per square meter of body-surface area) followed by gemcitabine (1000 mg per square meter) on days 1, 8, and 15 every 4 weeks or gemcitabine monotherapy (1000 mg per square meter) weekly for 7 of 8 weeks (cycle 1) and then on days 1, 8, and 15 every 4 weeks (cycle 2 and subsequent cycles). Patients received the study treatment until disease progression. The primary end point was overall survival; secondary end points were progression-free survival and overall response rate.
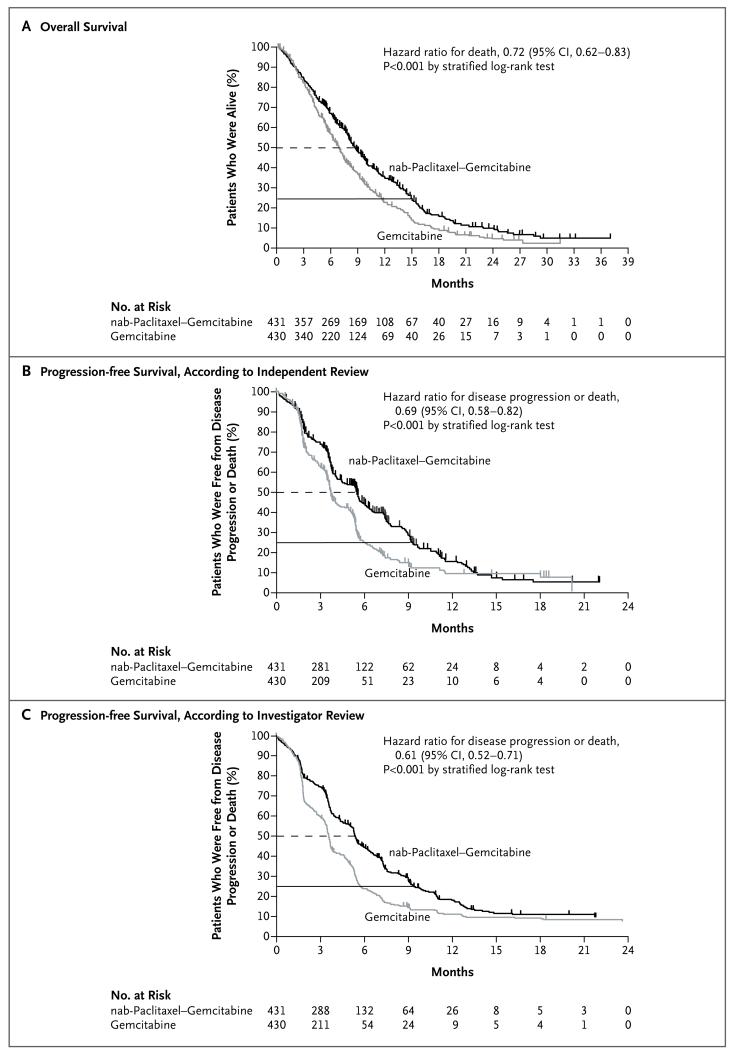
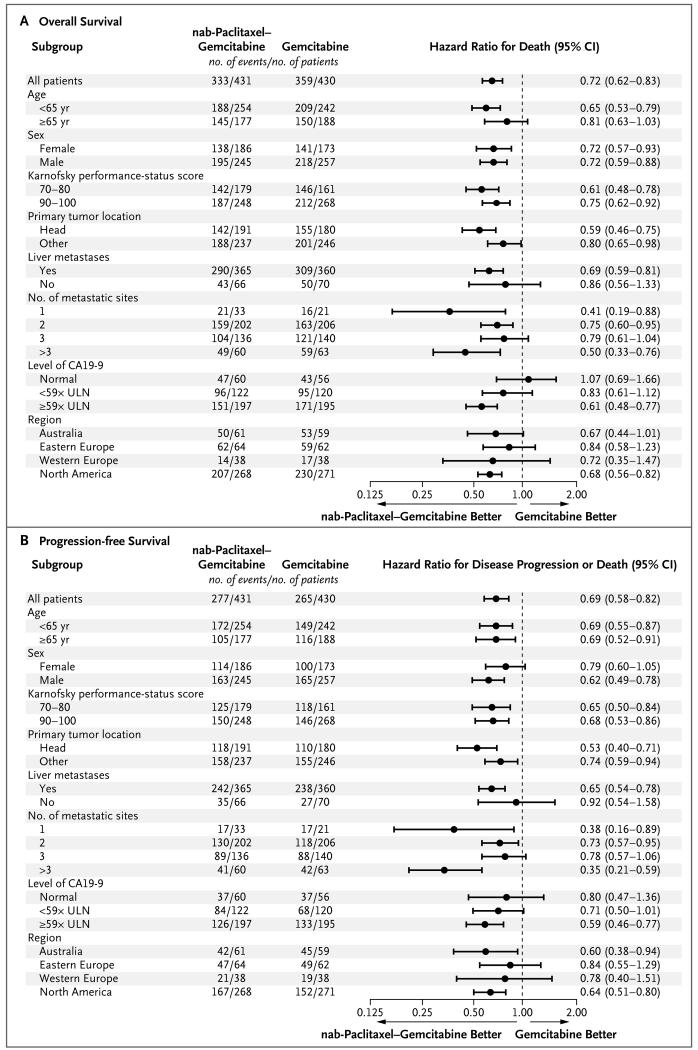
Results: A total of 861 patients were randomly assigned to nab-paclitaxel plus gemcitabine (431 patients) or gemcitabine (430). The median overall survival was 8.5 months in the nab-paclitaxel-gemcitabine group as compared with 6.7 months in the gemcitabine group (hazard ratio for death, 0.72; 95% confidence interval [CI], 0.62 to 0.83; P<0.001). The survival rate was 35% in the nab-paclitaxel-gemcitabine group versus 22% in the gemcitabine group at 1 year, and 9% versus 4% at 2 years. The median progression-free survival was 5.5 months in the nab-paclitaxel-gemcitabine group, as compared with 3.7 months in the gemcitabine group (hazard ratio for disease progression or death, 0.69; 95% CI, 0.58 to 0.82; P<0.001); the response rate according to independent review was 23% versus 7% in the two groups (P<0.001). The most common adverse events of grade 3 or higher were neutropenia (38% in the nab-paclitaxel-gemcitabine group vs. 27% in the gemcitabine group), fatigue (17% vs. 7%), and neuropathy (17% vs. 1%). Febrile neutropenia occurred in 3% versus 1% of the patients in the two groups. In the nab-paclitaxel-gemcitabine group, neuropathy of grade 3 or higher improved to grade 1 or lower in a median of 29 days.
Conclusions: In patients with metastatic pancreatic adenocarcinoma, nab-paclitaxel plus gemcitabine significantly improved overall survival, progression-free survival, and response rate, but rates of peripheral neuropathy and myelosuppression were increased. (Funded by Celgene; ClinicalTrials.gov number, NCT00844649.).
Figures
Comment in
-
Pancreatic cancer: standing on the shoulders of mice, making an iMPACT on pancreatic cancer.Nat Rev Clin Oncol. 2013 Dec;10(12):665. doi: 10.1038/nrclinonc.2013.209. Epub 2013 Nov 5. Nat Rev Clin Oncol. 2013. PMID: 24189469 No abstract available.
-
Albumin-bound paclitaxel plus gemcitabine in pancreatic cancer.N Engl J Med. 2014 Jan 30;370(5):479-80. doi: 10.1056/NEJMc1314761. N Engl J Med. 2014. PMID: 24476438 No abstract available.
-
Albumin-bound paclitaxel plus gemcitabine in pancreatic cancer.N Engl J Med. 2014 Jan 30;370(5):478. doi: 10.1056/NEJMc1314761. N Engl J Med. 2014. PMID: 24476439 No abstract available.
-
Albumin-bound paclitaxel plus gemcitabine in pancreatic cancer.N Engl J Med. 2014 Jan 30;370(5):478-9. doi: 10.1056/NEJMc1314761. N Engl J Med. 2014. PMID: 24476440 No abstract available.
-
New option for the initial management of metastatic pancreatic cancer?J Clin Oncol. 2014 Aug 10;32(23):2405-7. doi: 10.1200/JCO.2013.54.4155. Epub 2014 Jun 30. J Clin Oncol. 2014. PMID: 24982449 Free PMC article. No abstract available.
References
-
- Cancer facts and figures 2013. American Cancer Society; Atlanta: 2013.
-
- Malvezzi M, Bertuccio P, Levi F, La Vecchia C, Negri E. European cancer mortality predictions for the year 2013. Ann Oncol. 2013;24:792–800. - PubMed
-
- Burris HA, III, Moore MJ, Andersen J, et al. Improvements in survival and clinical benefit with gemcitabine as first-line therapy for patients with advanced pancreas cancer: a randomized trial. J Clin Oncol. 1997;15:2403–13. - PubMed
-
- Conroy T, Desseigne F, Ychou M, et al. FOLFIRINOX versus gemcitabine for metastatic pancreatic cancer. N Engl J Med. 2011;364:1817–25. - PubMed
-
- Moore MJ, Goldstein D, Hamm J, et al. Erlotinib plus gemcitabine compared with gemcitabine alone in patients with advanced pancreatic cancer: a phase III trial of the National Cancer Institute of Canada Clinical Trials Group. J Clin Oncol. 2007;25:1960–6. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical