

Amyloid-first and neurodegeneration-first profiles characterize incident amyloid PET positivity
- PMID: 24132377
- PMCID: PMC3821718
- DOI: 10.1212/01.wnl.0000435556.21319.e4
Amyloid-first and neurodegeneration-first profiles characterize incident amyloid PET positivity
Abstract
Objective: To estimate the incidence of and to characterize cognitive and imaging findings associated with incident amyloid PET positivity.
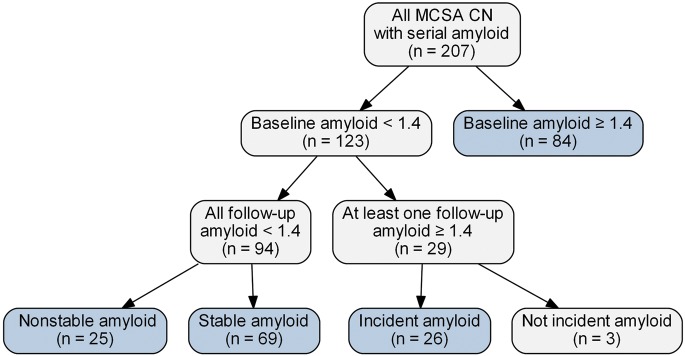
Methods: Cognitively normal (CN) participants in the Mayo Clinic Study of Aging who had 2 or more serial imaging assessments, which included amyloid PET, FDG-PET, and MRI at each time point, were eligible for analysis (n = 207). Twelve subjects with Alzheimer disease dementia were included for comparison.
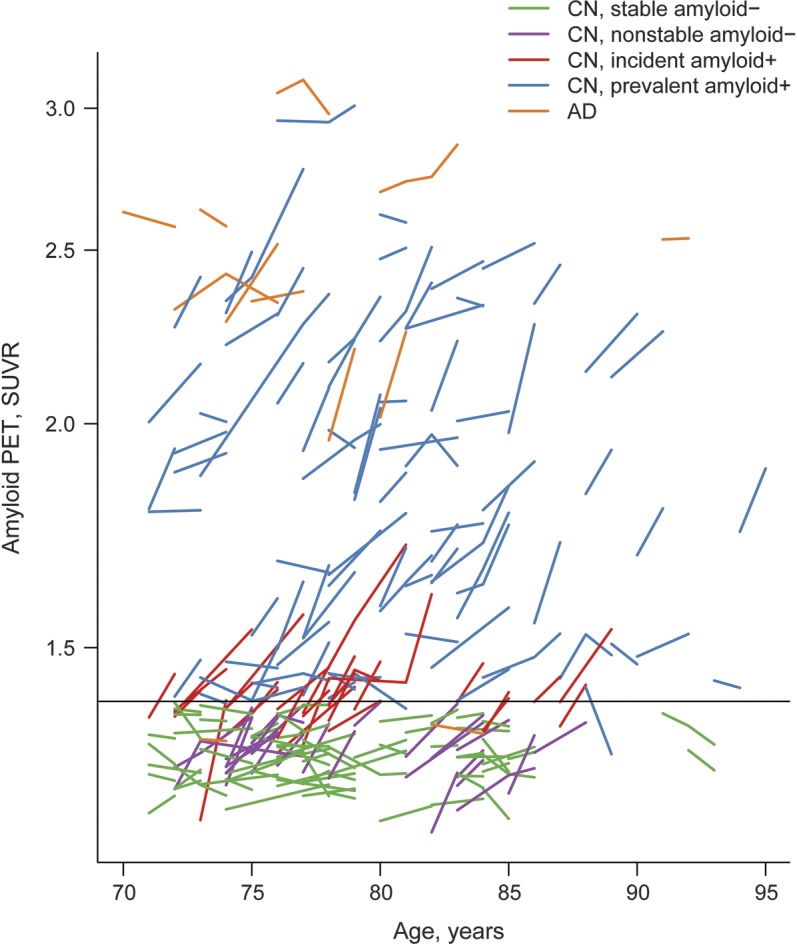
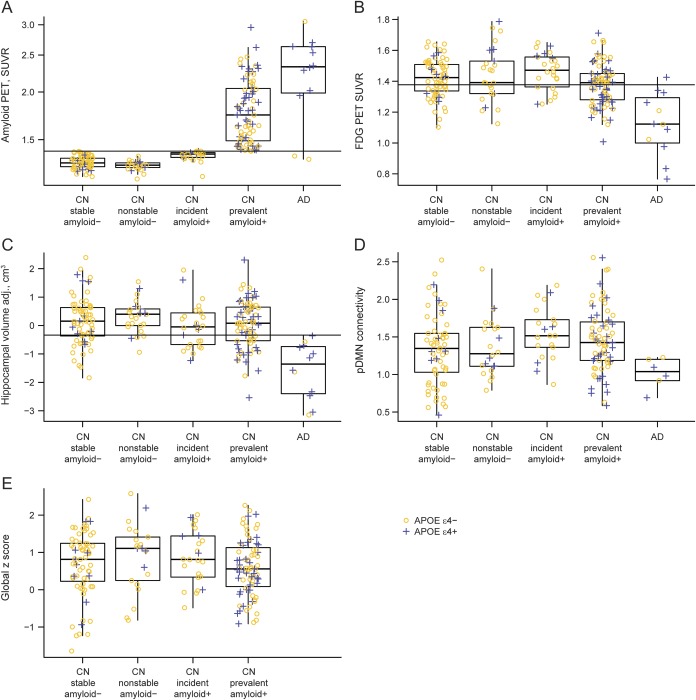
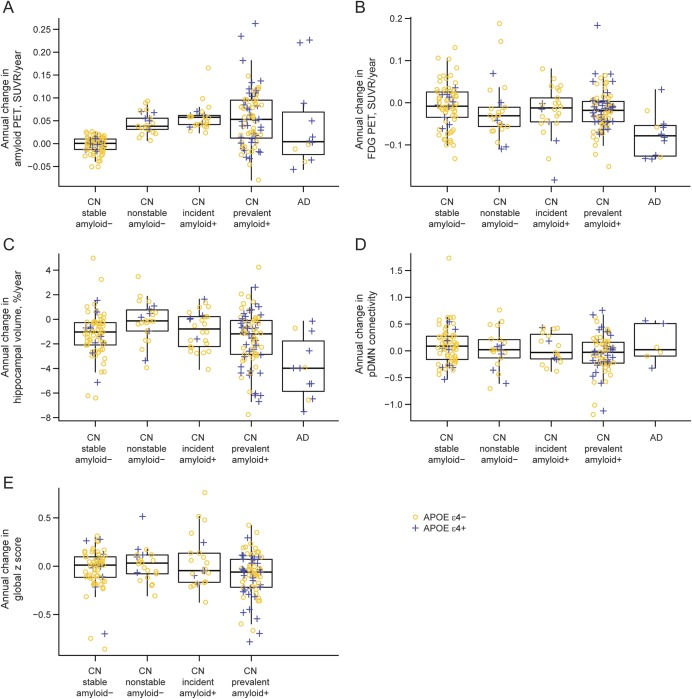
Results: Of the 123 CN participants who were amyloid-negative at baseline, 26 met criteria for incident amyloid PET positivity. Compared to the 69 subjects who remained stable amyloid-negative, on average these 26 did not differ on any imaging, demographic, or cognitive variables except amyloid PET (by definition) and task-free functional connectivity, which at baseline was greater in the incident amyloid-positive group. Eleven of the 26 incident amyloid-positive subjects had abnormal hippocampal volume, FDG-PET, or both at baseline.
Conclusions: The incidence of amyloid PET positivity is approximately 13% per year among CN participants over age 70 sampled from a population-based cohort. In 15/26 (58%), incident amyloid positivity occurred prior to abnormalities in FDG-PET and hippocampal volume. However, 11/26 (42%) incident amyloid-positive subjects had evidence of neurodegeneration prior to incident amyloid positivity. These 11 could be subjects with combinations of preexisting non-Alzheimer pathophysiologies and tau-mediated neurodegeneration who newly entered the amyloid pathway. Our findings suggest that both "amyloid-first" and "neurodegeneration-first" biomarker profile pathways to preclinical AD exist.
Figures
Comment in
-
Amyloid and neurodegeneration: converging and diverging paths.Neurology. 2013 Nov 12;81(20):1728-9. doi: 10.1212/01.wnl.0000435568.38352.2e. Epub 2013 Oct 16. Neurology. 2013. PMID: 24132372 No abstract available.
References
-
- Chetelat G, Villemagne VL, Villain N, et al. Accelerated cortical atrophy in cognitively normal elderly with high beta-amyloid deposition. Neurology 2012;78:477–484 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous