

Composite measures for profiling hospitals on bariatric surgery performance
- PMID: 24132708
- PMCID: PMC4163018
- DOI: 10.1001/jamasurg.2013.4109
Composite measures for profiling hospitals on bariatric surgery performance
Abstract
Importance: The optimal approach for profiling hospital performance with bariatric surgery is unclear.
Objective: To develop a novel composite measure for profiling hospital performance with bariatric surgery.
Design, setting, and participants: Using clinical registry data from the Michigan Bariatric Surgery Collaborative, we studied all patients undergoing bariatric surgery from January 1, 2008, through December 31, 2010. For laparoscopic gastric bypass surgery, we used empirical Bayes techniques to create a composite measure by combining several measures, including serious complications, reoperations, and readmissions; hospital and surgeon volume; and outcomes with other related procedures. Hospitals were ranked for 2008 through 2009 and placed in 1 of 3 groups: 3-star (top 20%), 2-star (middle 60%), and 1-star (bottom 20%). We assessed how well these ratings predicted outcomes in the next year (2010) compared with other widely used measures.
Main outcomes and measures: Risk-adjusted serious complications.
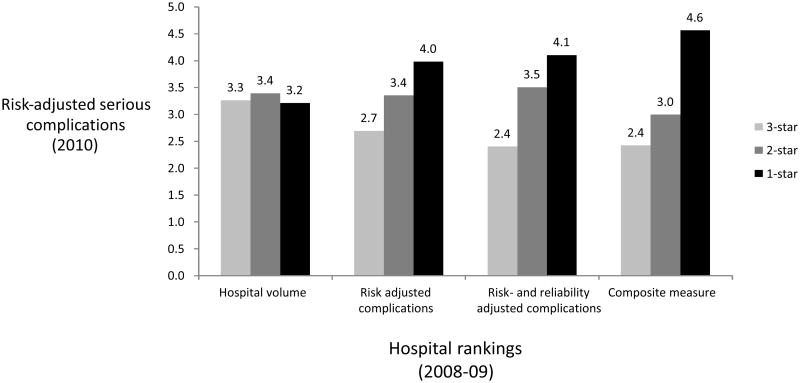
Results: Composite measures explained a larger proportion of hospital-level variation in serious complication rates with laparoscopic gastric bypass than other measures. For example, the composite measure explained 89% of the variation compared with only 28% for risk-adjusted complication rates alone. Composite measures also appeared better at predicting future performance compared with individual measures. When ranked on the composite measure, 1-star hospitals had 2-fold higher serious complication rates (4.6% vs 2.4%; odds ratio, 2.0; 95% CI, 1.1-3.5) compared with 3-star hospitals. Differences in serious complication rates between 1- and 3-star hospitals were much smaller when hospitals were ranked using serious complications (4.0% vs 2.7%; odds ratio, 1.6; 95% CI, 0.8-2.9) and hospital volume (3.3% vs 3.2%; odds ratio, 0.85; 95% CI, 0.4-1.7).
Conclusions and relevance: Composite measures are much better at explaining hospital-level variation in serious complications and predicting future performance than other approaches. In this preliminary study, it appears that such composite measures may be better than existing alternatives for profiling hospital performance with bariatric surgery.
Figures
Comment in
-
Hospital quality: does past performance predict future performance?JAMA Surg. 2014 Jan;149(1):16-7. doi: 10.1001/jamasurg.2013.4143. JAMA Surg. 2014. PMID: 24132658 No abstract available.
References
-
- Pratt GM, McLees B, Pories WJ. The ASBS Bariatric Surgery Centers of Excellence program: a blueprint for quality improvement. Surg Obes Relat Dis. 2006;2(5):497–503. discussion 503. - PubMed
-
- Schirmer B, Jones DB. The American College of Surgeons Bariatric Surgery Center Network: establishing standards. Bull Am Coll Surg. 2007;92(8):21–7. - PubMed
-
- Birkmeyer NJ, et al. Hospital complication rates with bariatric surgery in Michigan. JAMA. 2010;304(4):435–42. - PubMed
-
- Livingston EH. Bariatric surgery outcomes at designated centers of excellence vs nondesignated programs. Arch Surg. 2009;144(4):319–25. discussion 325. - PubMed
-
- Dimick JB, Welch HG, Birkmeyer JD. Surgical mortality as an indicator of hospital quality: the problem with small sample size. JAMA. 2004;292(7):847–51. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
