

Is chest CT useful in newborn screened infants with cystic fibrosis at 1 year of age?
- PMID: 24132911
- PMCID: PMC3963531
- DOI: 10.1136/thoraxjnl-2013-204176
Is chest CT useful in newborn screened infants with cystic fibrosis at 1 year of age?
Abstract
Rationale: Sensitive outcome measures applicable in different centres to quantify and track early pulmonary abnormalities in infants with cystic fibrosis (CF) are needed both for clinical care and interventional trials. Chest CT has been advocated as such a measure yet there is no validated scoring system in infants.
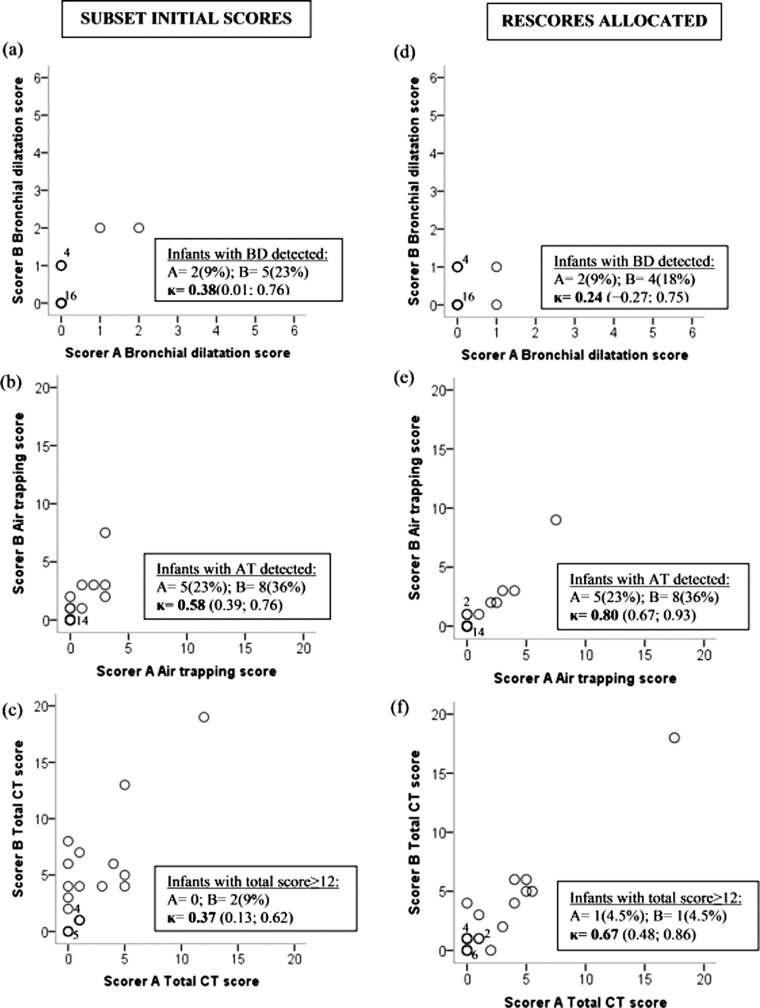
Objectives: The objectives of this study were to standardise CT data collection across multiple sites; ascertain the incidence of bronchial dilatation and air trapping in newborn screened (NBS) infants with CF at 1 year; and assess the reproducibility of Brody-II, the most widely used scoring system in children with CF, during infancy.
Methods: A multicentre observational study of early pulmonary lung disease in NBS infants with CF at age 1 year using volume-controlled chest CT performed under general anaesthetic.
Main results: 65 infants with NBS-diagnosed CF had chest CT in three centres. Small insignificant variations in lung recruitment manoeuvres but significant centre differences in radiation exposures were found. Despite experienced scorers and prior training, with the exception of air trapping, inter- and intraobserver agreement on Brody-II score was poor to fair (eg, interobserver total score mean (95% CI) κ coefficient: 0.34 (0.20 to 0.49)). Only 7 (11%) infants had a total CT score ≥ 12 (ie, ≥ 5% maximum possible) by either scorer.
Conclusions: In NBS infants with CF, CT changes were very mild at 1 year, and assessment of air trapping was the only reproducible outcome. CT is thus of questionable value in infants of this age, unless an improved scoring system for use in mild CF disease can be developed.
Figures
References
-
- Brody AS. Early morphologic changes in the lungs of asymptomatic infants and young children with cystic fibrosis. J Pediatr 2004;144:145–6 - PubMed
-
- Brody AS, Klein JS, Molina PL, et al. High-resolution computed tomography in young patients with cystic fibrosis: distribution of abnormalities and correlation with pulmonary function tests. J Pediatr 2004;145:32–8 - PubMed
-
- de Jong PA, Nakano Y, Lequin MH, et al. Progressive damage on high resolution computed tomography despite stable lung function in cystic fibrosis. Eur Respir J 2004;23:93–7 - PubMed
-
- Gustafsson PM, de Jong PA, Tiddens HA, et al. Multiple-breath inert gas washout and spirometry versus structural lung disease in cystic fibrosis. Thorax 2008;63:129–34 - PubMed
-
- Mott LS, Gangell CL, Murray CP, et al. Bronchiectasis in an asymptomatic infant with cystic fibrosis diagnosed following newborn screening. J Cyst Fibros 2009;8:285–7 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous