

Effects of ventricular insertion sites on rotational motion of left ventricular segments studied by cardiac MR
- PMID: 24133098
- PMCID: PMC3830433
- DOI: 10.1259/bjr.20130326
Effects of ventricular insertion sites on rotational motion of left ventricular segments studied by cardiac MR
Abstract
Objective: Obtaining new details for rotational motion of left ventricular (LV) segments using velocity encoding cardiac MR and correlating the regional motion patterns to LV insertion sites.
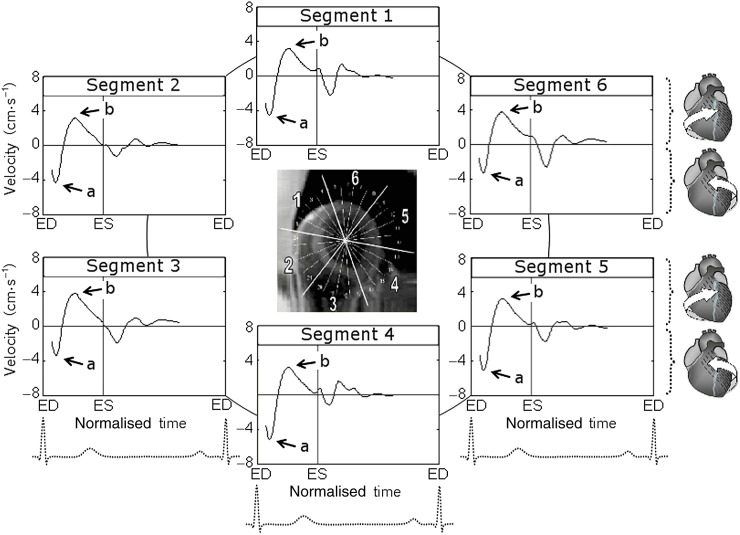
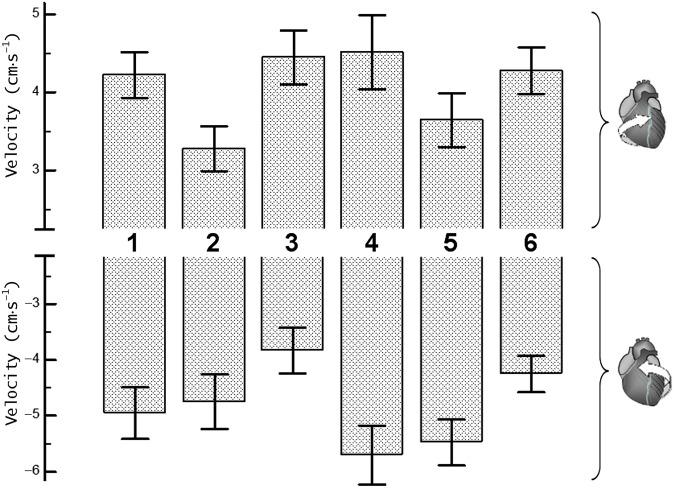
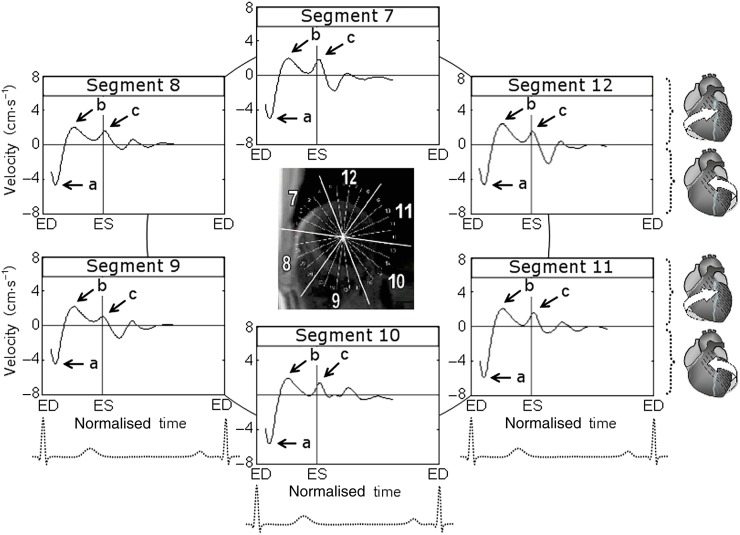
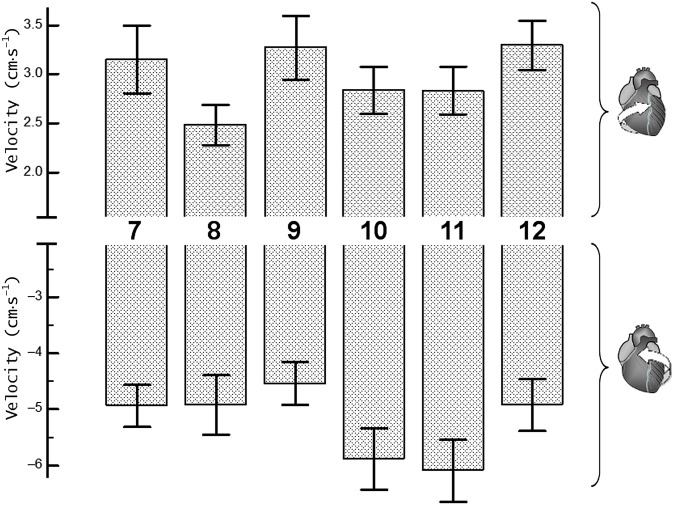
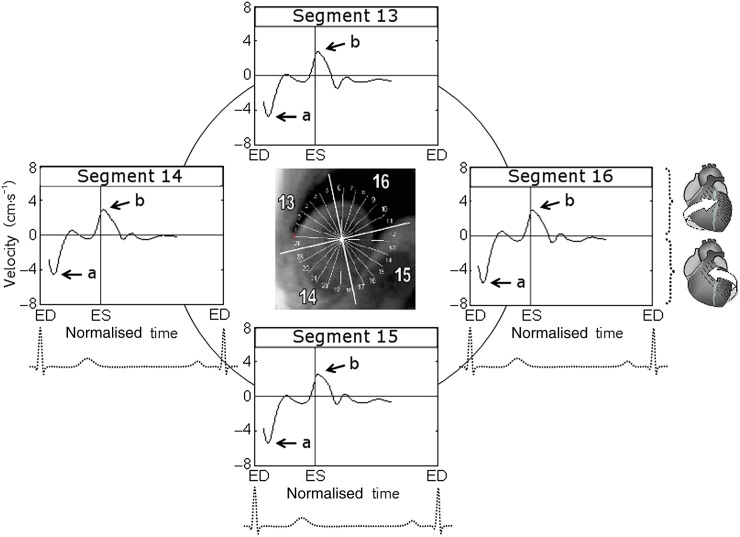
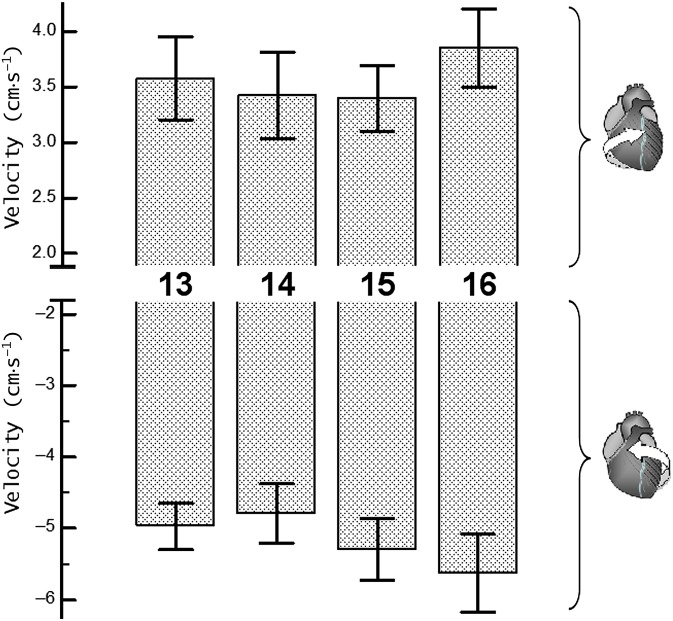
Methods: Cardiac MR examinations were performed on 14 healthy volunteers aged between 19 and 26 years. Peak rotational velocities and circumferential velocity curves were obtained for 16 ventricular segments.
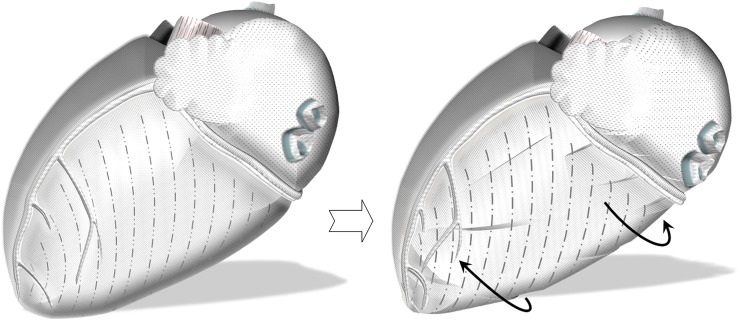
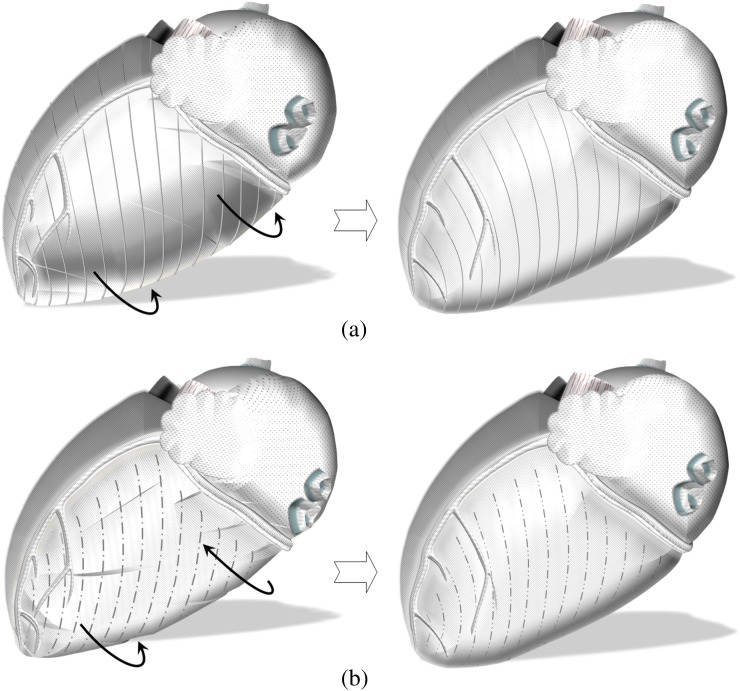
Results: Reduced peak clockwise velocities of anteroseptal segments (i.e. Segments 2 and 8) and peak counterclockwise velocities of inferoseptal segments (i.e. Segments 3 and 9) were the most prominent findings. The observations can be attributed to the LV insertion sites into the right ventricle, limiting the clockwise rotation of anteroseptal LV segments and the counterclockwise rotation of inferoseptal segments as viewed from the apex. Relatively lower clockwise velocities of Segment 5 and counterclockwise velocities of Segment 6 were also noted, suggesting a cardiac fixation point between these two segments, which is in close proximity to the lateral LV wall.
Conclusion: Apart from showing different rotational patterns of LV base, mid ventricle and apex, the study showed significant differences in the rotational velocities of individual LV segments. Correlating regional wall motion with known orientation of myocardial aggregates has also provided new insights into the mechanisms of LV rotational motions during a cardiac cycle.
Advances in knowledge: LV insertion into the right ventricle limits the clockwise rotation of anteroseptal LV segments and the counterclockwise rotation of inferoseptal segments adjacent to the ventricular insertion sites. The pattern should be differentiated from wall motion abnormalities in cardiac pathology.
Figures

Similar articles
-
Details of left ventricular radial wall motion supporting the ventricular theory of the third heart sound obtained by cardiac MR.Br J Radiol. 2014 May;87(1037):20130780. doi: 10.1259/bjr.20130780. Epub 2014 Feb 24. Br J Radiol. 2014. PMID: 24641347 Free PMC article.
-
Details of left ventricular remodeling and the mechanism of paradoxical ventricular septal motion after coronary artery bypass graft surgery.J Invasive Cardiol. 2011 Jul;23(7):276-82. J Invasive Cardiol. 2011. PMID: 21725122
-
Normal values of regional and global myocardial wall motion in young and elderly individuals using navigator gated tissue phase mapping.Age (Dordr). 2014 Feb;36(1):231-41. doi: 10.1007/s11357-013-9535-x. Epub 2013 Apr 21. Age (Dordr). 2014. PMID: 23604860 Free PMC article.
-
Assessment of systolic and diastolic LV function by MR myocardial tagging.Basic Res Cardiol. 1996;91 Suppl 2:23-8. doi: 10.1007/BF00795358. Basic Res Cardiol. 1996. PMID: 8957540 Review.
-
Prevalence of left ventricular 'rigid body rotation', the near absence of left ventricular twist (insights from the MAGYAR studies).Rev Cardiovasc Med. 2022 Jan 8;23(1):5. doi: 10.31083/j.rcm2301005. Rev Cardiovasc Med. 2022. PMID: 35092197 Review.
Cited by
-
Magnetic resonance tissue phase mapping demonstrates altered left ventricular diastolic function in children with chronic kidney disease.Pediatr Radiol. 2017 Feb;47(2):169-177. doi: 10.1007/s00247-016-3741-5. Epub 2016 Dec 13. Pediatr Radiol. 2017. PMID: 27966039
-
Details of left ventricular radial wall motion supporting the ventricular theory of the third heart sound obtained by cardiac MR.Br J Radiol. 2014 May;87(1037):20130780. doi: 10.1259/bjr.20130780. Epub 2014 Feb 24. Br J Radiol. 2014. PMID: 24641347 Free PMC article.
References
-
- Gustafsson U, Lindqvist P, Morner S, Waldenstrom A. Assessment of regional rotation patterns improves the understanding of the systolic and diastolic left ventricular function: an echocardiographic speckle-tracking study in healthy individuals. Eur J Echocardiogr 2009;10:56–61 10.1093/ejechocard/jen141 - DOI - PubMed
-
- Maier SE, Fischer SE, McKinnon GC, Hess OM, Krayenbuehl HP, Boesiger P. Evaluation of left ventricular segmental wall motion in hypertrophic cardiomyopathy with myocardial tagging. Circulation 1992;86:1919–28 - PubMed
-
- Kroeker CA, Tyberg JV, Beyar R. Effects of ischemia on left ventricular apex rotation. An experimental study in anesthetized dogs. Circulation 1995;92:3539–48 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
