

The role of non-invasive positive pressure ventilation in post-extubation respiratory failure: An evaluation using meta-analytic techniques
- PMID: 24133337
- PMCID: PMC3796908
- DOI: 10.4103/0972-5229.118477
The role of non-invasive positive pressure ventilation in post-extubation respiratory failure: An evaluation using meta-analytic techniques
Abstract
Background: The use of non-invasive positive pressure ventilation (NIPPV) in post-extubation respiratory failure is not well-established. Meta-analytic techniques were used to assess the effects of prophylactic application of NIPPV (prior to the development of respiratory failure) and therapeutic application of NIPPV (subsequent to the development of respiratory failure).
Materials and methods: Randomized controlled trials (RCTs) from 1966 to May 2010 were identified using electronic databases. RCTs, which reported the use of NIPPV in post-extubation respiratory failure with defined assessable endpoints: reintubation, mortality and length of stay, were included.
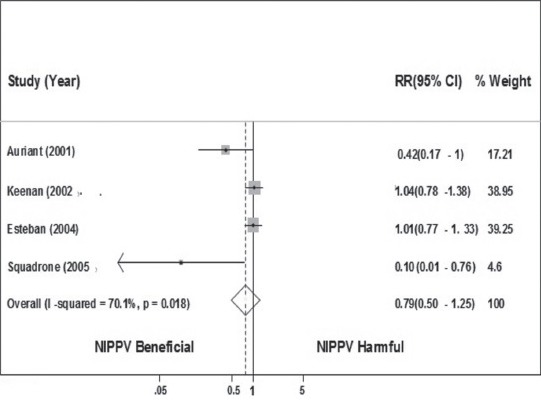
Results: Reintubation was the primary outcome, mortality and lengths of stay were the secondary outcomes. Risk ratios (RR) were calculated for discrete outcomes and weighted mean differences (WMD) for continuous measures. There were 13 trials with 1420 patients; 9 prophylactic with 861 patients and 4 therapeutic with 559 patients. In the prophylactic group, NIPPV was associated with lower rates of reintubation: RR 0.53 (95% confidence interval [CI], 0.28-0.98), P = 0.04. In the therapeutic group, NIPPV showed a null effect on reintubation: RR 0.79 (95% CI, 0.50-1.25), P = 0.31. The analysis on the secondary outcomes suggested significant reduction of hospital mortality with prophylactic application of NIPPV: RR 0.62 (95% CI 0.4-0.97), P = 0.03, with no effect on the other outcomes. Therapeutic application of NIPPV reduced intensive care unit length of stay: WMD -1.17 (95% CI -2.82 to -0.33), P = 0.006, but no effect on the other secondary outcomes.
Conclusions: The results of this review suggested prophylactic NIPPV was beneficial with respect to reintubation and the therapeutic use of NIPPV showed a null effect.
Keywords: Bi-level positive airway pressure ventilation; continuous positive airway pressure ventilation; non-invasive ventilation; post-extubation; reintubation; respiratory failure.
Conflict of interest statement
Figures


Similar articles
-
Prehospital noninvasive positive pressure ventilation for severe respiratory distress in adult patients: An updated meta-analysis.J Clin Nurs. 2022 Dec;31(23-24):3327-3337. doi: 10.1111/jocn.16224. Epub 2022 Feb 24. J Clin Nurs. 2022. PMID: 35212078 Review.
-
[A meta-analysis of nasal intermittent positive pressure ventilation in treatment of respiratory distress syndrome in premature infants].Zhonghua Er Ke Za Zhi. 2009 Jul;47(7):532-6. Zhonghua Er Ke Za Zhi. 2009. PMID: 19951518 Chinese.
-
Randomized Controlled Trial of Nonsynchronized Nasal Intermittent Positive Pressure Ventilation versus Nasal CPAP after Extubation of VLBW Infants.Neonatology. 2020;117(2):193-199. doi: 10.1159/000506164. Epub 2020 May 8. Neonatology. 2020. PMID: 32388511 Clinical Trial.
-
Nasal HFOV versus nasal IPPV as a post-extubation respiratory support in preterm infants-a randomised controlled trial.Eur J Pediatr. 2021 Oct;180(10):3151-3160. doi: 10.1007/s00431-021-04084-1. Epub 2021 Apr 23. Eur J Pediatr. 2021. PMID: 33890156 Free PMC article. Clinical Trial.
-
Use of NHFOV vs. NIPPV for the respiratory support of preterm newborns after extubation: A meta-analysis.Front Pediatr. 2023 Jan 11;10:1063387. doi: 10.3389/fped.2022.1063387. eCollection 2022. Front Pediatr. 2023. PMID: 36714640 Free PMC article. Review.
Cited by
-
Noninvasive Ventilation and Oxygen Therapy after Extubation in Patients with Acute Respiratory Failure: A Meta-analysis of Randomized Controlled Trials.Indian J Crit Care Med. 2019 Sep;23(9):414-422. doi: 10.5005/jp-journals-10071-23236. Indian J Crit Care Med. 2019. PMID: 31645827 Free PMC article.
-
The role of non-invasive ventilation used immediately after planned extubation for adults with chronic respiratory disorders.Saudi Med J. 2018 Feb;39(2):131-136. doi: 10.15537/smj.2018.2.21942. Saudi Med J. 2018. PMID: 29436560 Free PMC article. Review.
-
Meta-analysis: Adding apples and oranges?Indian J Crit Care Med. 2014 Jan;18(1):50-1. doi: 10.4103/0972-5229.125444. Indian J Crit Care Med. 2014. PMID: 24550619 Free PMC article. No abstract available.
-
Helmet CPAP revisited in COVID-19 pneumonia: A case series.Can J Respir Ther. 2020 Jul 23;56:32-34. doi: 10.29390/cjrt-2020-019. eCollection 2020. Can J Respir Ther. 2020. PMID: 32844113 Free PMC article.
References
-
- Esteban A, Frutos F, Tobin MJ, Alía I, Solsona JF, Valverdú I, et al. A comparison of four methods of weaning patients from mechanical ventilation. Spanish Lung Failure Collaborative Group. N Engl J Med. 1995;332:345–50. - PubMed
-
- Brochard L, Rauss A, Benito S, Conti G, Mancebo J, Rekik N, et al. Comparison of three methods of gradual withdrawal from ventilatory support during weaning from mechanical ventilation. Am J Respir Crit Care Med. 1994;150:896–903. - PubMed
-
- Ely EW, Baker AM, Dunagan DP, Burke HL, Smith AC, Kelly PT, et al. Effect on the duration of mechanical ventilation of identifying patients capable of breathing spontaneously. N Engl J Med. 1996;335:1864–9. - PubMed
-
- Esteban A, Alía I, Gordo F, Fernández R, Solsona JF, Vallverdú I, et al. Extubation outcome after spontaneous breathing trials with T-tube or pressure support ventilation. The Spanish Lung Failure Collaborative Group. Am J Respir Crit Care Med. 1997;156:459–65. - PubMed
-
- Esteban A, Alía I, Tobin MJ, Gil A, Gordo F, Vallverdú I, et al. Effect of spontaneous breathing trial duration on outcome of attempts to discontinue mechanical ventilation. Spanish Lung Failure Collaborative Group. Am J Respir Crit Care Med. 1999;159:512–8. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources