

CHADS2 versus CHA2DS2-VASc score in assessing the stroke and thromboembolism risk stratification in patients with atrial fibrillation: a systematic review and meta-analysis
- PMID: 24133514
- PMCID: PMC3796700
- DOI: 10.3969/j.issn.1671-5411.2013.03.004
CHADS2 versus CHA2DS2-VASc score in assessing the stroke and thromboembolism risk stratification in patients with atrial fibrillation: a systematic review and meta-analysis
Abstract
Objective: To perform a systematic review and meta-analysis of the predictive abilities of CHADS2 and CHA2DS2-VASc in stroke and thromboembolism risk stratification of atrial fibrillation (AF) patients.
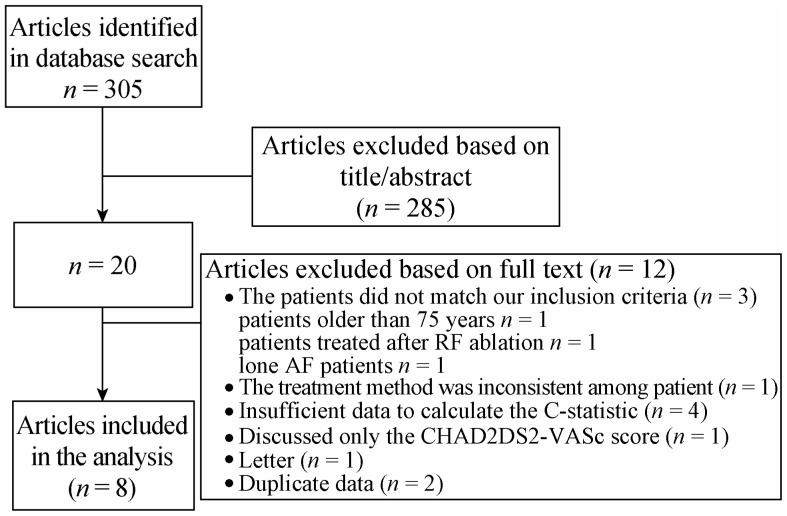
Methods: We searched PubMed and EMBASE for English-language literature on comparisons of the diagnostic performance between CHADS2 and CHA2DS2-VASc in predicting stroke, or systemic embolism, in AF. We then assessed the quality of the included studies and pooled the C-statistics and 95% confidence intervals (95% CI).
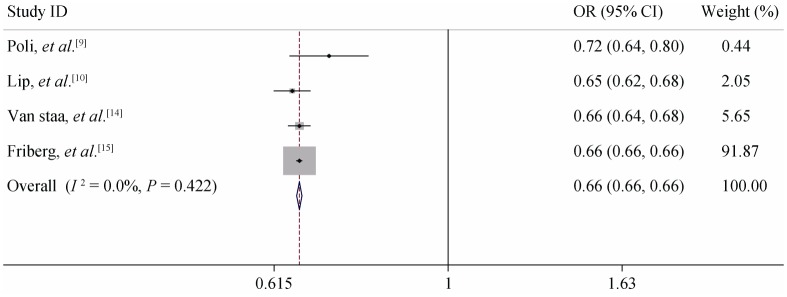
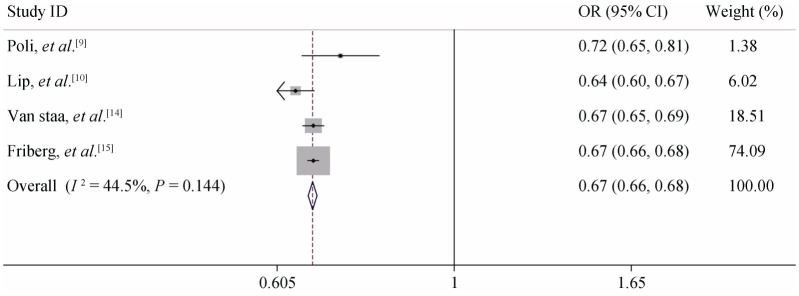
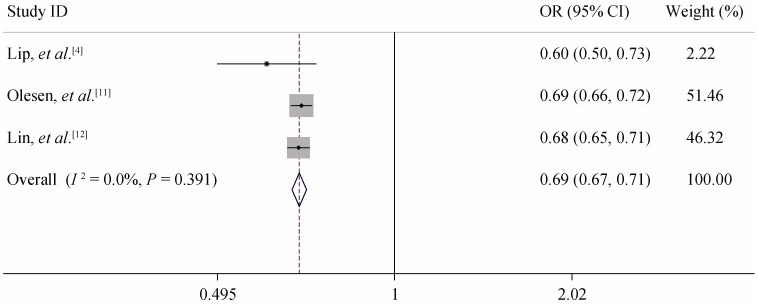
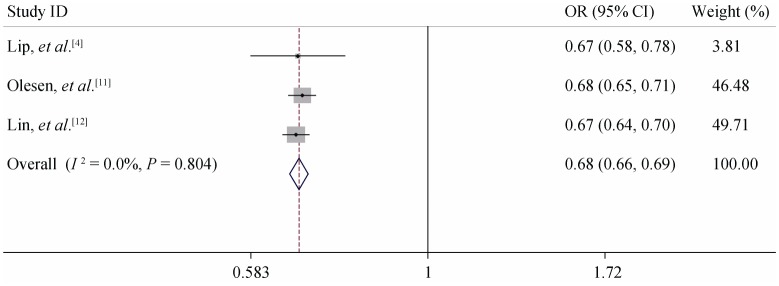
Results: Eight studies were included. It was unsuitable to perform a direct meta-analysis because of high heterogeneity. When analyzed as a continuous variable, the C-statistic ranged from 0.60 to 0.80 (median 0.683) for CHADS2 and 0.64-0.79 (median 0.673) for CHA2DS2-VASc. When analyzed as a continuous variable in anticoagulation patients, the subgroup analysis showed that the pooled C-statistic (95% CI) was 0.660 (0.655-0.665) for CHADS2 and 0.667 (0.651-0.683) for CHA2DS2-VASc (no significant difference). For non-anticoagulation patients, the pooled C-statistic (95% CI) was 0.685 (0.666-0.705) for CHADS2 and 0.675 (0.656-0.694) for CHA2DS2-VASc (no significant difference). The average ratio of endpoint events in the low-risk group of CHA2DS2-VASc was less than CHADS2 (0.41% vs. 0.94%, P < 0.05). The average proportion of the moderate-risk group of CHA2DS2-VASc was lower than CHADS2 (11.12% vs. 30.75%, P < 0.05).
Conclusions: The C-statistic suggests a similar clinical utility of the CHADS2 and CHA2DS2-VASc scores in predicting stroke and thromboembolism, but CHA2DS2- VASc has the important advantage of identifying extremely low-risk patients with atrial fibrillation, as well as classifying a lower proportion of patients as moderate risk.
Keywords: Atrial fibrillation; CHA2DS2-VASc; CHADS2; Meta-analysis; Prediction; Stroke.
Figures
References
-
- [No authors listed] Risk factors for stroke and efficacy of antithrombotic therapy in atrial fibrillation: analysis of pooled data from five randomized controlled trials. Arch Intern Med. 1994;154:1449–1457. - PubMed
-
- Lip GY, Edwards SJ. Stroke prevention with aspirin warfarin and ximelagatran in patients with non-valvular atrial fibrillation: A system review and meta-analysis. Thromb Res. 2006;118:321–333. - PubMed
-
- Gage BF, Waterman AD, Shannon W, et al. et al. validation of clinical classification schemes for predicting stroke: results of the National Registry of Atrial Fibrillation. JAMA. 2001;285:2864–2870. - PubMed
-
- Lip GY, Nieuwlaat R, Pisters R, et al. et al. Refining clinical risk stratification for predicting stroke and thromboembolism in atrial fibrillation using a novel risk factor-based approach: the euro heart survey on atrial fibrillation. Chest. 2010;137:263–272. - PubMed
-
- Camm AJ, Lip GY, De Caterina R, et al. et al. 2012 focused update of the ESC Guidelines for the management of atrial fibrillation: An update of the 2010 ESC Guidelines for the management of atrial fibrillation. Europace. 2012;14:1385–1413. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources