

Adult patients with nosocomial pneumonia: epidemiology, diagnosis, and treatment
- PMID: 24133545
- PMCID: PMC3796359
- DOI: 10.3238/arztebl.2013.0634
Adult patients with nosocomial pneumonia: epidemiology, diagnosis, and treatment
Abstract
Background: Nosocomial pneumonia is among the most common types of infection in hospitalized patients. The increasing prevalence of multi-drug resistant organisms (MDROs) in recent years points to the need for an up-to-date clinical guideline.
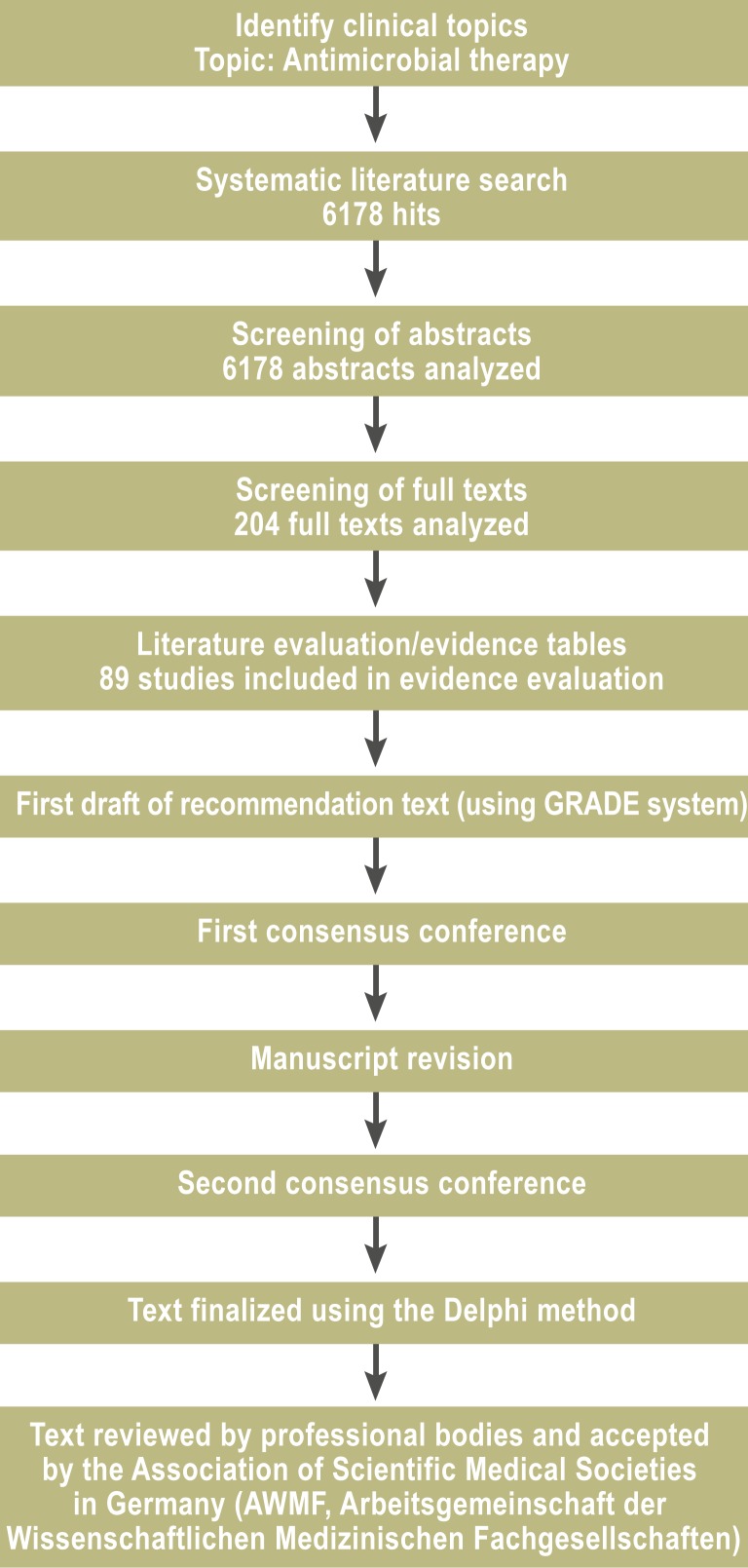
Methods: An interdisciplinary S3 guideline was created on the basis of a systematic literature review in the PubMed and Cochrane Library databases, with assessment and grading of the evidence according to the GRADE system.
Results: 9097 abstracts and 808 articles were screened in full text, and 22 recommendations were issued. It is recommended that any antimicrobial treatment should be preceded by a microbiological diagnostic evaluation with cultures of blood and respiratory samples. The diagnosis of nosocomial pneumonia should be suspected in any patient with a new or worsened pulmonary infiltrate who meets any two of the following three criteria: leucocyte count above 10,000 or below 4000/µL, temperature above 38.3°C, and/or the presence of purulent respiratory secretions. The initially calculated antimicrobial treatment should be begun without delay; it should be oriented to the locally prevailing resistance pattern, and its intensity should be a function of the risk of infection with MDROs. The initial treatment should be combination therapy if there is a high risk of MDRO infection and/or if the patient is in septic shock. In the new guideline, emphasis is laid on a strict de-escalation concept. In particular, antimicrobial treatment usually should not be continued for longer than eight days.
Conclusion: The new guideline's recommendations are intended to encourage rational use of antibiotics, so that antimicrobial treatment will be highly effective while the unnecessary selection of multi-drug-resistant organisms will be avoided.
Figures
Comment in
-
Nosocomial infections - a present and future challenge.Dtsch Arztebl Int. 2013 Sep;110(38):625-6. doi: 10.3238/arztebl.2013.0625. Dtsch Arztebl Int. 2013. PMID: 24133542 Free PMC article. No abstract available.
-
In reply.Dtsch Arztebl Int. 2014 Jan 6;111(1-2):10-1. doi: 10.3238/arztebl.2014.0010b. Dtsch Arztebl Int. 2014. PMID: 24565271 Free PMC article. No abstract available.
-
The crucial role of molecular diagnostics.Dtsch Arztebl Int. 2014 Jan 6;111(1-2):10. doi: 10.3238/arztebl.2014.0010a. Dtsch Arztebl Int. 2014. PMID: 24565272 Free PMC article. No abstract available.
References
-
- Ewig S, Welte T, Chastre J, et al. Rethinking the concepts of community-acquired and health-care-associated pneumonia. Lancet Infect Dis. 2010;10:279–287. - PubMed
-
- Dalhoff K, Marxsen J, Steinhoff J. Pneumonien bei Immunsuppression. Internist. 2007;48:507–518. - PubMed
-
- Meyer E, Sohr D, Gastmeier P, et al. New identification of outliers and ventilator-associated pneumonia rates from 2005 to 2007 within the German Nosocomial Infection Surveillance System. J Hosp Infect. 2009;73:246–252. - PubMed
-
- Muscedere JG, Day A, Heyland DK. Mortality, attributable mortality, and clinical events as end points for clinical trials of ventilator-associated pneumonia and hospital-acquired pneumonia. Clin Infect Dis. 2010;51:120–125. - PubMed
-
- Gatermann S, Kaase M. Nachweis von Carbapenemasen 2010. Epidemiol Bull. 2011;32:301–304.
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical