

Do pre-hospital anaesthesiologists reliably predict mortality using the NACA severity score? A retrospective cohort study
- PMID: 24134443
- PMCID: PMC4287201
- DOI: 10.1111/aas.12208
Do pre-hospital anaesthesiologists reliably predict mortality using the NACA severity score? A retrospective cohort study
Abstract
Introduction: The National Advisory Committee on Aeronautics' (NACA) severity score is widely used in pre-hospital emergency medicine to grade the severity of illness or trauma in patient groups but is scarcely validated. The aim of this study was to assess the score's ability to predict mortality and need for advanced in-hospital interventions in a cohort from one anaesthesiologist-manned helicopter service in Northern Norway.
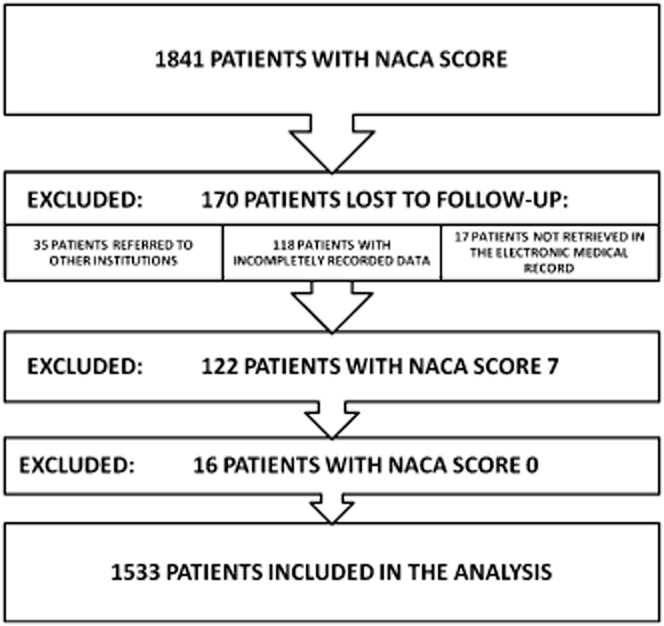
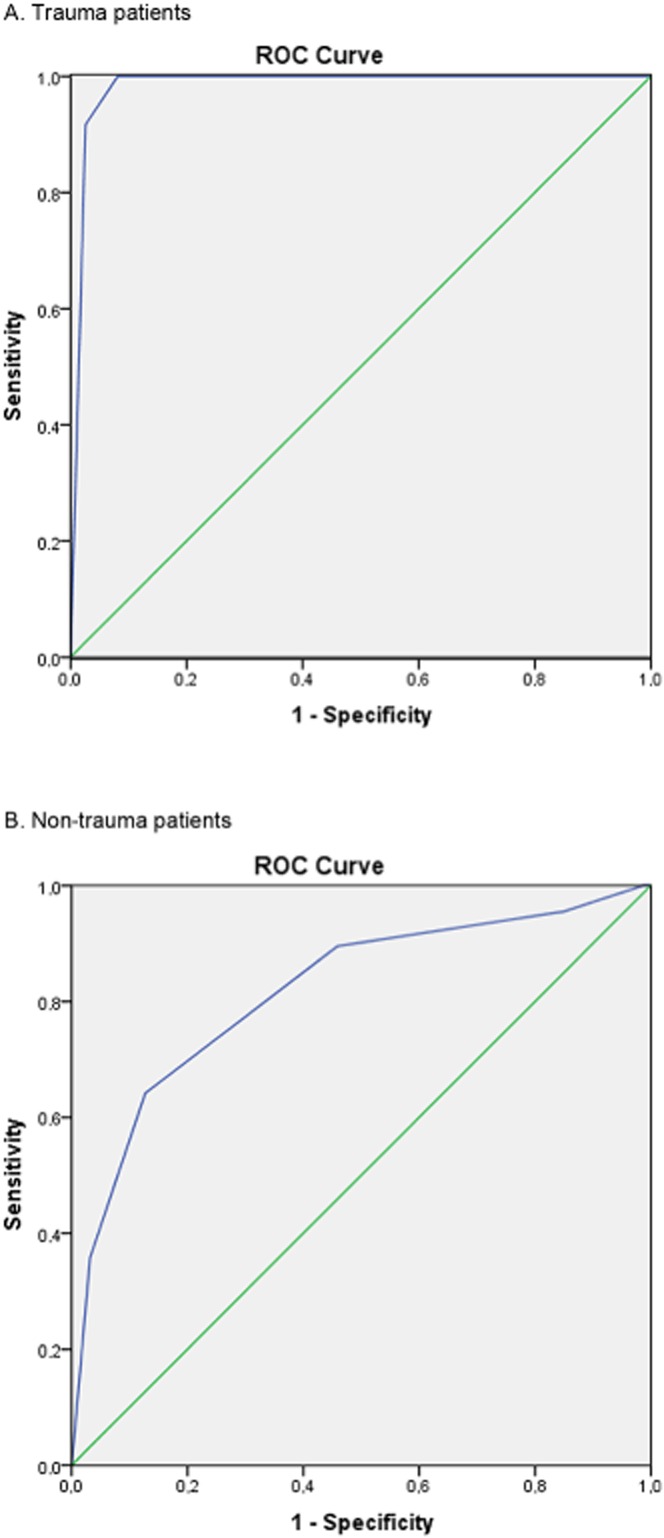
Methods: All missions completed by one helicopter service during January 1999 to December 2009 were reviewed. One thousand eight hundred forty-one patients were assessed by the NACA score. Pre-hospital and in-hospital interventions were collected from patient records. The relationship between NACA score and the outcome measures was assessed using receiver operating characteristic (ROC) curves.
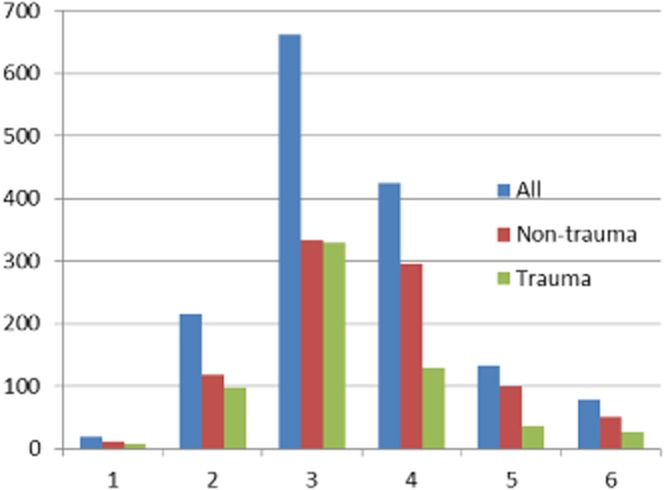
Results: A total of 1533 patients were included in the analysis; uninjured and dead victims were excluded per protocol. Overall mortality rate of the patients with NACA score 1-6 was 5.2%. Trauma patients with NACA score 1-6 had overall mortality rate of 1.9% (12/625) and non-trauma patients 7.4% (67/908). The NACA score's ability to predict mortality was assessed by using ROC area under curve (AUC) and was 0.86 for all, 0.82 for non-trauma and 0.98 for trauma patients. The NACA score's ability to predict a need for respiratory therapy within 24 h revealed an AUC of 0.90 for all patients combined.
Conclusion: The NACA score had good discrimination for predicting mortality and need for respiratory therapy. It is thus useful as a tool to measure overall severity of the patient population in this kind of emergency medicine system.
© 2013 The Acta Anaesthesiologica Scandinavica Foundation. Published by John Wiley & Sons Ltd.
Figures
References
-
- Statistisches Bundesamt Wiesbaden. Handbuch der Internationalen Klassifikation der Krankheiten, Verletzungen und Todesursachen, 8. Revision. Bd. I: Systematisches Verzeichnis. Stuttgart Mainz: Kohlhammer; 1968.
-
- Weiss M, Bernoulli L, Zollinger A. Der NACA-Index. Der NACA-Index. Aussagekraft und Stellenwert des modifizierten NACA-Indexes in der präklinischen Schweregraderfassung von Unfallpatienten. Anaesthesist. 2001;50:150–154. - PubMed
-
- Tryba M, Brüggemann H, Echtermeyr V. Klassifizierung von Erkrankungen und Verletzungen im Notarztrettungssystem. Notfallmedizin. 1980;8:725–727.
-
- Bonatti J, Göschl O, Larcher P, Wödlinger R, Flora G. Predictors of short-term survival after helicopter rescue. Resuscitation. 1995;30:133–140. - PubMed
-
- Fredriksen K. An overview of air medical transport in Norway. In: Blumen I, Lemkin DL, Brozen R, Doyle TJ, Dries DJ, Petersen P, Robinson KJ, Romig L, Swanson ER, Williams KA, editors. Principles and direction of Air Medical Transport. Salt Lake City: Air Medical Physician Association; 2006. pp. 657–660.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
