

doi: 10.1186/gm499.
eCollection 2013.
The Coriell personalized medicine collaborative pharmacogenomics appraisal, evidence scoring and interpretation system
Affiliations
- PMID: 24134832
- PMCID: PMC3978656
- DOI: 10.1186/gm499
Item in Clipboard
The Coriell personalized medicine collaborative pharmacogenomics appraisal, evidence scoring and interpretation system
Genome Med.
.
Abstract
Implementation of pharmacogenomics (PGx) in clinical care can lead to improved drug efficacy and reduced adverse drug reactions. However, there has been a lag in adoption of PGx tests in clinical practice. This is due in part to a paucity of rigorous systems for translating published clinical and scientific data into standardized diagnostic tests with clear therapeutic recommendations. Here we describe the Pharmacogenomics Appraisal, Evidence Scoring and Interpretation System (PhAESIS), developed as part of the Coriell Personalized Medicine Collaborative research study, and its application to seven commonly prescribed drugs.
Figures
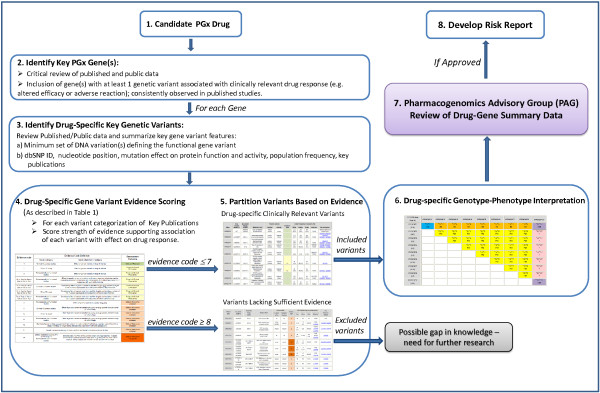
Schematic representation of the Coriell Personalized Medicine Collaborative (CPMC) Pharmacogenomics Appraisal, Evidence-based Scoring and Interpretation System (PhAESIS) Procedure. Candidate drugs for PGx reporting are identified and prioritized for the CPMC study based on a number of criteria (as listed in the Methods section). Once a drug is selected for evaluation, the FDA drug label, the peer-reviewed scientific and clinical literature, and public web-based databases are searched for studies that report drug-related genotype–phenotype associations (see Additional file 1: Table S1 for examples of resources). This initial search identifies genes with a significant influence on response to this drug, with at least one genetic variant that is significantly and consistently associated with a clinically relevant drug-response outcome (altered efficacy or adverse reaction). For each key PGx gene, drug-specific gene variant evidence scoring is carried out (as described in the Methods section) using the scale depicted in Table 1. Genetic variant evidence scores are used to partition variants based on potential clinical relevance. Scores of 7 or lower indicate a defined effect on drug response or clinical outcome, whereas those of 8 or higher represent a lack of or insufficient evidence for an effect. Once all of the genetic variants of potential clinical relevance (those with evidence codes ≤7) have been identified, the anticipated response of the diploid individual (who possesses two copies of the gene, one inherited from each parent) with each combination of inherited variants is defined, based on published clinical outcomes data. A Punnett square is used to represent distinct diploid individuals, each assigned a defined drug response phenotype. Curated data from steps 2 to 6 are prepared as PhAESIS summary documents for review by the CPMC Pharmacogenomics Advisory Group (PAG). If approved by the PAG, drug-specific risk reports are then developed and released to study participants.
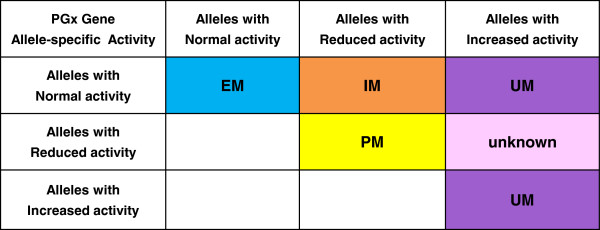
Example of a simple Punnett square providing general rules for assignment of predicted drug-specific response phenotypes for a particular drug-metabolizing pharmacogenomics (PGx) gene. Annotation of pharmacokinetics/pharmacodynamics (PK/PD) outcome: EM, extensive metabolizers; IM, intermediate metabolizers; PM, poor metabolizers; UM, ultra-rapid metabolizers; unknown, drug metabolizing phenotype currently unknown. Note that for other types of PGx genes such as drug transporters, the PK/PD phenotype can be similarly annotated in the Punnett square table, for example as ‘normal’ for normal transport; ‘decreased’ for reduced transport; and ‘increased’ for increased transport. Annotation of the associated clinical outcome: shades of blue indicate ‘normal’ response to the drug; yellow, most extreme adverse drug reaction (ADR) or altered efficacy resulting from deficiency or reduced function/activity of the PGx protein product; orange, clinically distinct or milder adverse drug reaction/altered efficacy resulting from protein deficiency or reduced function; purple, distinct ADR or altered efficacy resulting from excess or increased function of the protein product; pink, unknown phenotype for the defined diplotype. The group of diplotypes with unknown phenotype represent a gap in knowledge where further research is warranted.
References
LinkOut - more resources
Full Text Sources
Other Literature Sources
