

Prenatal diagnosis, birth location, surgical center, and neonatal mortality in infants with hypoplastic left heart syndrome
- PMID: 24135071
- PMCID: PMC7302400
- DOI: 10.1161/CIRCULATIONAHA.113.003711
Prenatal diagnosis, birth location, surgical center, and neonatal mortality in infants with hypoplastic left heart syndrome
Abstract
Background: Most studies have not demonstrated improved survival after prenatal diagnosis of critical congenital heart disease, including hypoplastic left heart syndrome (HLHS). However, the effect of delivery near a cardiac surgical center (CSC), the recommended action after prenatal diagnosis, on HLHS mortality has been poorly investigated.
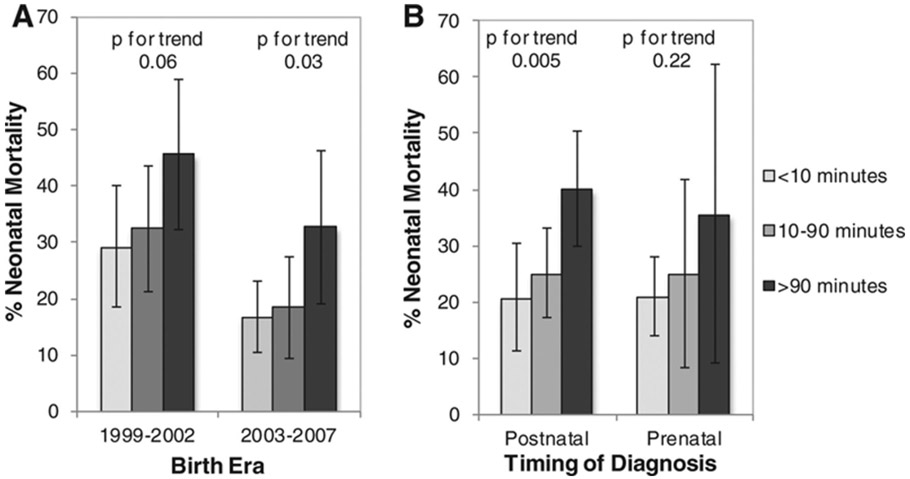
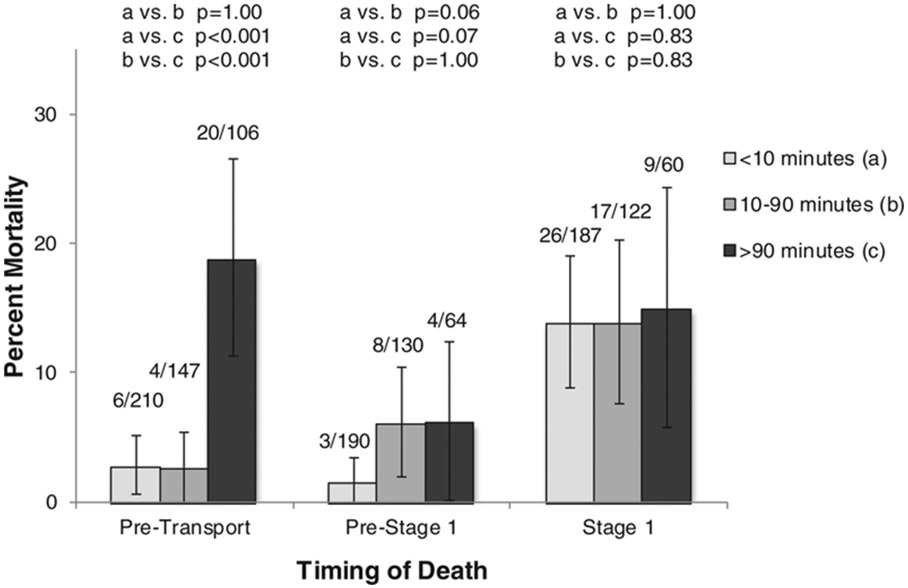
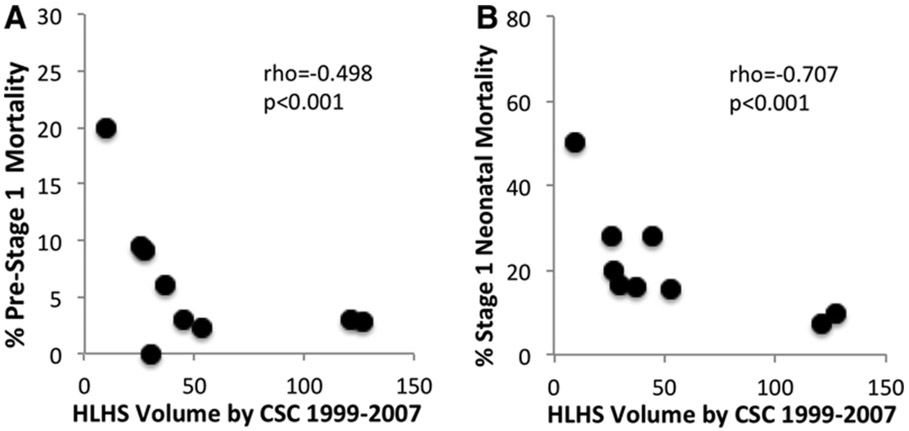
Methods and results: Using Texas Birth Defects Registry data, 1999 through 2007, which monitored >3.4 million births, we investigated the association between distance (calculated driving time) from birth center to CSC and neonatal mortality in 463 infants with HLHS. Infants with extracardiac birth defects or genetic disorders were excluded. The associations between prenatal diagnosis, CSC HLHS volume, and mortality were also examined. Neonatal mortality in infants born <10 minutes from a CSC was 21.0%, 10 to 90 minutes 25.2%, and >90 minutes 39.6% (P for trend <0.001). Prenatal diagnosis alone was not associated with improved survival (P=0.14). In multivariable analysis, birth >90 minutes from a CSC remained associated with increased mortality (odds ratio, 2.03; 95% confidence interval, 1.19-3.45), compared with <10 minutes. In subanalysis, birth >90 minutes from a CSC was associated with higher pretransport mortality (odds ratio, 6.69; 95% confidence interval, 2.52-17.74) and birth 10 to 90 minutes with higher presurgical mortality (odds ratio, 4.45; 95% confidence interval, 1.17-17.00). Higher surgical mortality was associated with lower CSC HLHS volume (odds ratio per 10 patients, 0.88; 95% confidence interval, 0.84-0.91).
Conclusions: Infants with HLHS born far from a CSC have increased neonatal mortality, and most of this mortality is presurgical. Efforts to improve prenatal diagnosis of HLHS and subsequent delivery near a large volume CSC may significantly improve neonatal HLHS survival.
Keywords: heart defects, congenital; hypoplastic left heart syndrome; mortality; population; prenatal diagnosis.
Conflict of interest statement
Figures
References
-
- Members Writing Group, Roger VL, Go AS, Lloyd-Jones DM, Benjamin EJ, Berry JD, Borden WB, Bravata DM, Dai S, Ford ES, Fox CS, Fullerton HJ, Gillespie C, Hailpern SM, Heit JA, Howard VJ, Kissela BM, Kittner SJ, Lackland DT, Lichtman JH, Lisabeth LD, Makuc DM, Marcus GM, Marelli A, Matchar DB, Moy CS, Mozaffarian D, Mussolino ME, Nichol G, Paynter NP, Soliman EZ, Sorlie PD, Sotoodehnia N, Turan TN, Virani SS, Wong ND, Woo D, Turner MB, on behalf of the American Heart Association Statistics Committee and Stroke Statistics Subcommittee, On behalf of the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart Disease and Stroke Statistics--2012 Update: A Report From the American Heart Association. Circulation. 2012;125:e2–e220. - PMC - PubMed
-
- Boneva RS, Botto LD, Moore CA, Yang Q, Correa A, Erickson JD. Mortality Associated With Congenital Heart Defects in the United States : Trends and Racial Disparities, 1979–1997. Circulation. 2001;103:2376–2381. - PubMed
-
- Kuehl KS, Loffredo CA, Ferencz C. Failure to diagnose congenital heart disease in infancy. Pediatrics. 1999;103:743–747. - PubMed
-
- Feinstein JA, Benson DW, Dubin AM, Cohen MS, Maxey DM, Mahle WT, Pahl E, Villafañe J, Bhatt AB, Peng LF, Johnson BA, Marsden AL, Daniels CJ, Rudd NA, Caldarone CA, Mussatto KA, Morales DL, Ivy DD, Gaynor JW, Tweddell JS, Deal BJ, Furck AK, Rosenthal GL, Ohye RG, Ghanayem NS, Cheatham JP, Tworetzky W, Martin GR. Hypoplastic Left Heart Syndrome. J Am Coll Cardiol.. 2012;59:S1–S42. - PMC - PubMed
-
- Verheijen PM, Lisowski LA, Stoutenbeek P, Hitchcock JF, Brenner JI, Copel JA, Kleinman CS, Meijboom EJ, Bennink GBWE. Prenatal diagnosis of congenital heart disease affects preoperative acidosis in the newborn patient. J Thorac Cardiovasc Surg. 2001;121:798–803. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
