

Prognostic impact of tumour-infiltrating immune cells on biliary tract cancer
- PMID: 24136146
- PMCID: PMC3833207
- DOI: 10.1038/bjc.2013.610
Prognostic impact of tumour-infiltrating immune cells on biliary tract cancer
Abstract
Background: Biliary tract cancers (BTC) are relatively rare malignant tumours with poor prognosis. It is known from other solid neoplasms that antitumour inflammatory response has an impact on tumour behaviour and patient outcome. The aim of this study was to provide a comprehensive characterisation of antitumour inflammatory response in human BTC.
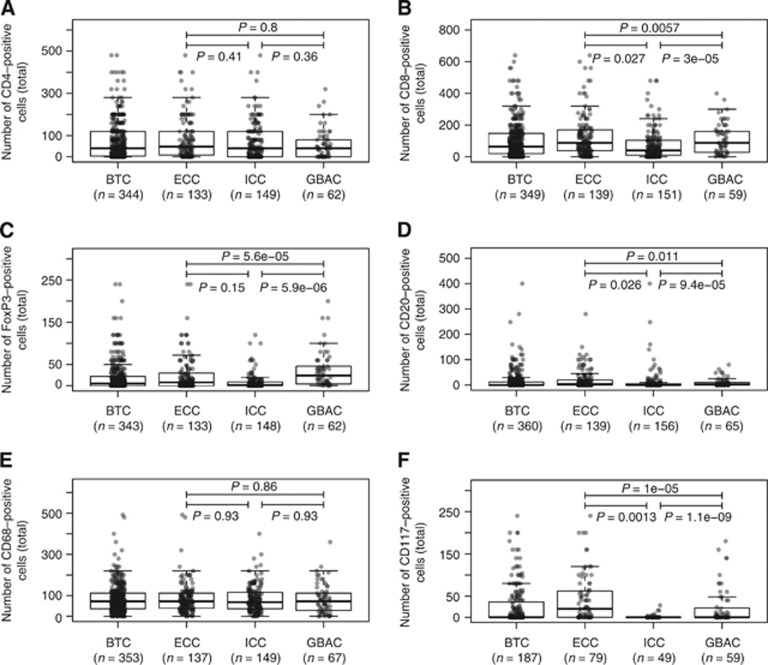
Methods: Tumour-infiltrating T lymphocytes (CD4+, CD8+, and Foxp3+), natural killer cells (perforin+), B lymphocytes (CD20+), macrophages (CD68+) as well as mast cells (CD117+) were assessed by immunohistochemistry in 375 BTC including extrahepatic (ECC; n=157), intrahepatic (ICC; n=149), and gallbladder (GBAC; n=69) adenocarcinomas. Overall and intraepithelial quantity of tumour-infiltrating immune cells was analysed. Data were correlated with clinicopathological variables and patient survival.
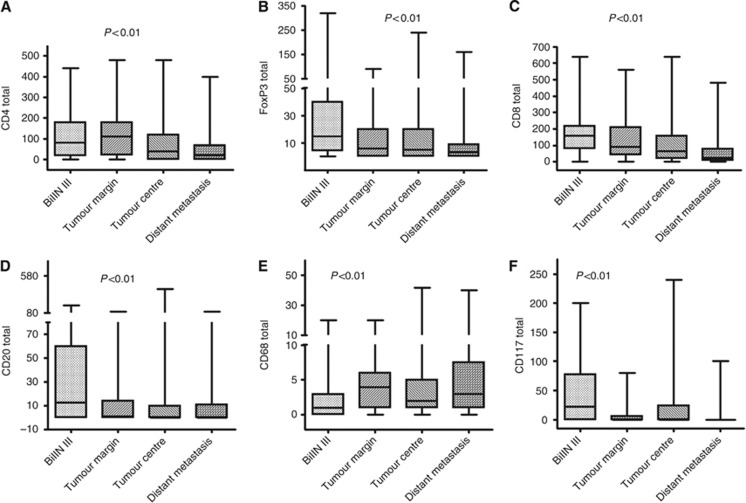
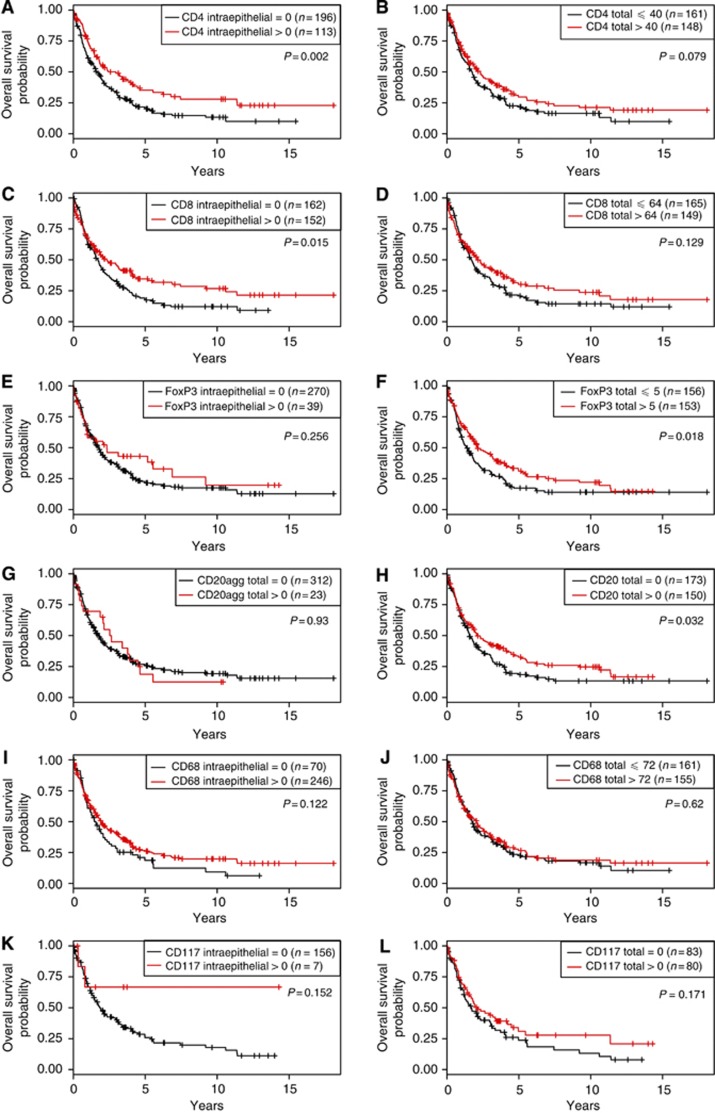
Results: The most prevalent inflammatory cell type in BTC was the T lymphocyte. Components of the adaptive immune response decreased, whereas innate immune response components increased significantly in the biliary intraepithelial neoplasia - primary carcinoma - metastasis sequence. BTC patients with intraepithelial tumour-infiltrating CD4+, CD8+, and Foxp3+ T lymphocytes showed a significantly longer overall survival. Number of total intraepithelial tumour-infiltrating Foxp3+ regulatory T lymphocytes (HR: 0.492, P=0.002) and CD4+ T lymphocytes (HR: 0.595, P=0.008) were tumour grade- and UICC-stage-independent prognosticators. The subtype-specific evaluation revealed that the tumour-infiltrating lymphocytic infiltrate is a positive outcome predictor in ECC and GBAC but not in ICC.
Conclusion: Our findings characterise the immune response in cholangiocarcinogenesis and identify inflammatory cell types that influence the outcome of BTC patients. Further, we show that BTC subtypes show relevant differences with respect to density, quality of inflammation, and impact on patient survival.
Figures
Similar articles
-
Major histocompatibility complex class I expression impacts on patient survival and type and density of immune cells in biliary tract cancer.Br J Cancer. 2015 Nov 3;113(9):1343-9. doi: 10.1038/bjc.2015.337. Epub 2015 Oct 13. Br J Cancer. 2015. PMID: 26461054 Free PMC article.
-
The intratumoural subsite and relation of CD8(+) and FOXP3(+) T lymphocytes in colorectal cancer provide important prognostic clues.Br J Cancer. 2014 May 13;110(10):2551-9. doi: 10.1038/bjc.2014.161. Epub 2014 Mar 27. Br J Cancer. 2014. PMID: 24675384 Free PMC article.
-
DMBT1 expression in biliary carcinogenesis with correlation of clinicopathological data.Histopathology. 2017 Jun;70(7):1064-1071. doi: 10.1111/his.13175. Epub 2017 Mar 28. Histopathology. 2017. PMID: 28130841
-
The prognostic value of tumour-infiltrating lymphocytes in pancreatic cancer: a systematic review and meta-analysis.Eur J Cancer. 2020 Jun;132:71-84. doi: 10.1016/j.ejca.2020.03.013. Epub 2020 Apr 22. Eur J Cancer. 2020. PMID: 32334338
-
Prognostic roles nutritional index in patients with resectable and advanced biliary tract cancers.World J Gastroenterol. 2025 Feb 14;31(6):97697. doi: 10.3748/wjg.v31.i6.97697. World J Gastroenterol. 2025. PMID: 39958446 Free PMC article.
Cited by
-
Impact of perioperative blood transfusion on long-term survival in patients with different stages of perihilar cholangiocarcinoma treated with curative resection: A multicentre propensity score matching study.Front Oncol. 2022 Oct 31;12:1059581. doi: 10.3389/fonc.2022.1059581. eCollection 2022. Front Oncol. 2022. PMID: 36387093 Free PMC article.
-
Role of Chemokines in the Biology of Cholangiocarcinoma.Cancers (Basel). 2020 Aug 7;12(8):2215. doi: 10.3390/cancers12082215. Cancers (Basel). 2020. PMID: 32784743 Free PMC article. Review.
-
Identification of tumor antigens and immune subtypes of cholangiocarcinoma for mRNA vaccine development.Mol Cancer. 2021 Mar 8;20(1):50. doi: 10.1186/s12943-021-01342-6. Mol Cancer. 2021. PMID: 33685460 Free PMC article.
-
Cholangiocarcinoma 2020: the next horizon in mechanisms and management.Nat Rev Gastroenterol Hepatol. 2020 Sep;17(9):557-588. doi: 10.1038/s41575-020-0310-z. Epub 2020 Jun 30. Nat Rev Gastroenterol Hepatol. 2020. PMID: 32606456 Free PMC article. Review.
-
The Expression of Programmed Death-Ligand 1 on Immune Cells Is Related to a Better Prognosis in Biliary Tract Cancer.Gut Liver. 2023 Nov 15;17(6):933-941. doi: 10.5009/gnl220206. Epub 2022 Dec 13. Gut Liver. 2023. PMID: 36510775 Free PMC article.
References
-
- Boon T, Cerottini JC, Van den Eynde B, van der Bruggen P, Van Pel A. Tumor antigens recognized by T lymphocytes. Ann Rev Immunol. 1994;12:337–365. - PubMed
-
- Bosman FT, Carneiro F, Hruban RH, Theise ND.2010WHO Classification of Tumours of the Digestive System4th ednInternational Agency for Research on Cancer (IARC): Lyon, France
-
- Brahmer JR, Tykodi SS, Chow LQ, Hwu WJ, Topalian SL, Hwu P, Drake CG, Camacho LH, Kauh J, Odunsi K, Pitot HC, Hamid O, Bhatia S, Martins R, Eaton K, Chen S, Salay TM, Alaparthy S, Grosso JF, Korman AJ, Parker SM, Agrawal S, Goldberg SM, Pardoll DM, Gupta A, Wigginton JM. Safety and activity of anti-PD-L1 antibody in patients with advanced cancer. N Engl J Med. 2012;366 (26:2455–2465. - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
